Part 1. Introduction
Pediatric obesity has escalated into a critical global public health emergency. Current epidemiological projections estimate that by the year 2030, approximately 254 million children and adolescents worldwide will be affected by this condition. Obesity is not merely a concern of aesthetics or body image; it is a complex metabolic state that significantly elevates the risk of early-onset Type 2 diabetes, cardiovascular pathophysiology, and markedly diminishes the overall quality of life (QoL) for the developing individual.
The Current Treatment Landscape
The standard therapeutic approach—often referred to as the “triad” of nutritional management, physical activity, and behavioral modification—frequently encounters substantial barriers in clinical practice. These challenges include high rates of sedentary behavior among youth and physical maladaptation to high-intensity exercise regimens, which can lead to poor adherence and dropout.
![The Impact of Yoga on Pediatric Obesity [RESEARCH DECODED]](https://yogaismylife.vn/en/wp-content/uploads/2026/02/The-Impact-of-Yoga-on-Pediatric-Obesity.avif)
In this context, Yoga, characterized as a complementary Mind-Body intervention, is anticipated to serve as a safer, more sustainable alternative. It offers the distinct advantages of a lower risk profile for musculoskeletal injury and higher accessibility for this specific demographic compared to high-impact sports.
However, a critical question remains for the evidence-based practitioner: What is the actual, quantifiable efficacy of Yoga on “hard endpoints” such as BMI (Body Mass Index) or Body Fat Percentage in the pediatric population? This latest meta-analysis aims to clarify these physiological outcomes.
Study Overview
- Original Title: The Impact of Yoga Practices on Body Composition and Vital Signs in Children and Adolescents With Obesity: A Systematic Review and Meta-Analysis.
- Authors: Nuray Caner, Gülyeter Erdoğan Yüce.
- Publication Year: 2025 (May – Online ahead of print).
- Source: Obesity Reviews.
- Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC12404879/
- DOI: 10.1111/obr.13947

Why This Study Matters
- Specific Population: The study isolates the 10–24 age group (children, adolescents, and young adults). This is a critical demographic that is often resistant to adult-centric interventions and requires tailored therapeutic strategies.
- Latest Data: The review synthesizes the most current evidence, including studies updated through June 2024.
- Objectivity: The authors employed the RoB 2 (Risk of Bias 2) tool to rigorously assess methodological quality, ensuring that the findings are based on high-integrity scientific data.
Part 2. Objectives and Hypotheses
Primary Objectives
The study aims to synthesize quantitative evidence regarding the efficacy of Yoga interventions on specific anthropometric and hemodynamic parameters:
- Body Composition:
- BMI (kg/m^2)
- Absolute Body Weight (kg)
- Body Fat Percentage (%)
- Vital Signs:
- Heart Rate (HR)
- Blood Pressure (BP)
Scientific Hypothesis
The proposed mechanism of Yoga extends beyond simple caloric expenditure via physical movement (Asana). It is hypothesized that Yoga modulates the autonomic nervous system (ANS) through breath regulation (Pranayama) and meditation techniques. The hypothesis posits that Yoga reduces sympathetic arousal (stress reduction), thereby facilitating weight management and potentially contributing to improvements comparable to certain control conditions.
Part 3. Methodology
Study Design
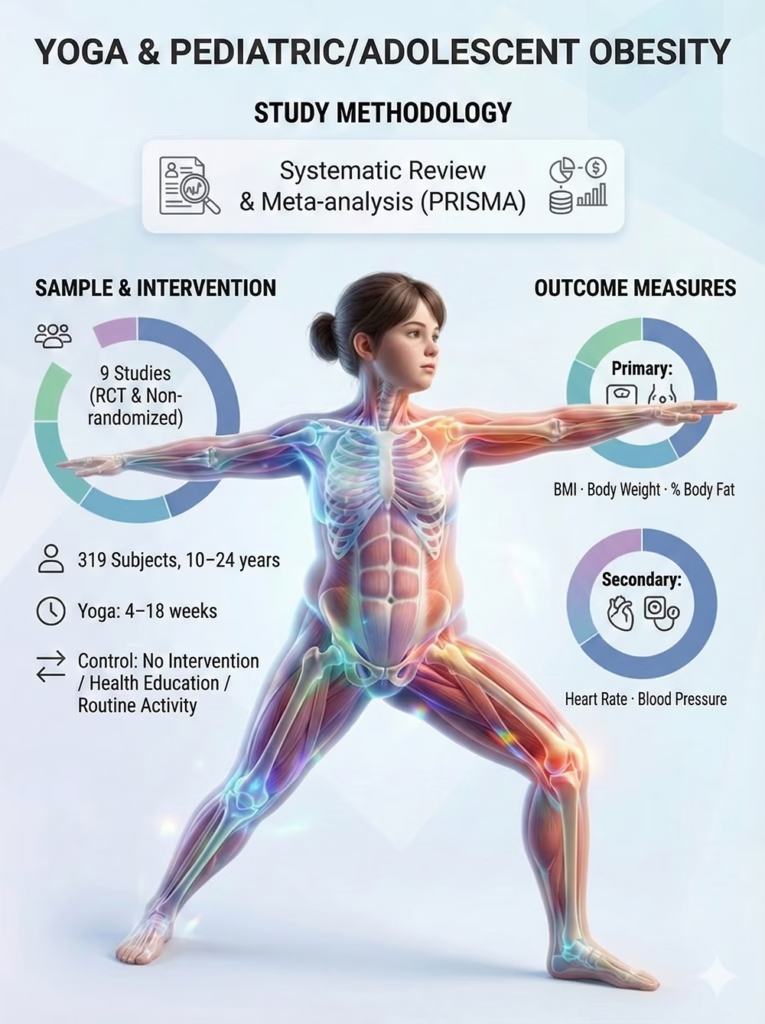
This is a Systematic Review and Meta-analysis, conducted in strict accordance with the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) to ensure transparency and reproducibility.
Subjects and Criteria
- Source: A total of 9 studies were included, comprising both Randomized Controlled Trials (RCTs) and non-randomized clinical trials. The geographic distribution includes India, China, the USA, South Korea, and Thailand, offering a diverse cross-cultural perspective.
- Sample Size: 319 participants, with a mean age ranging from 10 to 24 years.
- Intervention: Yoga practice protocols varied in duration from 4 weeks to 18 weeks, capturing both acute and sub-acute adaptations.
- Control Group: Interventions were compared against passive controls (no intervention), health education only, or standard physical education (PE) curricula.
Outcome Measures
- Primary Outcomes: Anthropometric indices including BMI ($kg/m^2$), Absolute Weight (kg), and Body Fat Percentage (%).
- Secondary Outcomes: Hemodynamic markers including Resting Heart Rate, Systolic Blood Pressure, and Diastolic Blood Pressure.
Part 4. Results – Deep Analysis of Clinical Significance
1. BMI Reduction: More Than Just a Number
The pooled analysis revealed a mean reduction of −1.09 kg/m². While this figure may appear numerically modest in absolute terms, it carries substantial clinical significance within the pediatric context.
Previous literature indicates that a BMI reduction of approximately 4–5% is sufficient to induce measurable improvements in:
- Insulin sensitivity and glucose homeostasis.
- Early markers of cardiovascular risk.
- Functional mobility and body confidence/self-efficacy.

Notable findings from the analysis:
- This efficacy was achieved solely with Yoga, without the addition of other exercise modalities.
- No High-Intensity Interval Training (HIIT) was required to achieve these results.
- No musculoskeletal injuries were reported, underscoring the safety profile.
- Conclusion: For pediatric populations, this level of improvement may be clinically meaningful and sufficient to support long-term adherence.”
2. Body Fat Percentage Reduction: “Quality” over Quantity
A statistically significant reduction of −1.62% in body fat percentage was observed. This suggests that Yoga may influence body fat composition rather than merely causing fluctuations in water weight.
This is critical for metabolic health because:
- Visceral and subcutaneous fat depots are the primary drivers of chronic low-grade inflammation and metabolic syndrome.
- BMI alone acts as a surrogate marker and does not accurately reflect metabolic risk or body composition changes.
- Implication: Yoga may contribute to favorable changes in body composition (increased lean mass ratio), even if total body weight does not drop precipitously.

3. Unchanged Body Weight: A Positive Outcome?
The finding that absolute body weight did not show a statistically significant decrease is not a therapeutic failure, but rather a clinically important observation.
In the pediatric and adolescent population:
- The body is in an active growth phase.
- The clinical goal is often weight maintenance or the deceleration of weight gain (improving the growth trajectory) rather than rapid weight loss, which can impact linear growth.
- Maintaining weight while reducing Body Fat % $\rightarrow$ Clinical Success.
- This approach mitigates the risk of eating disorders, weight obsession, and the adverse effects of aggressive caloric restriction on development.

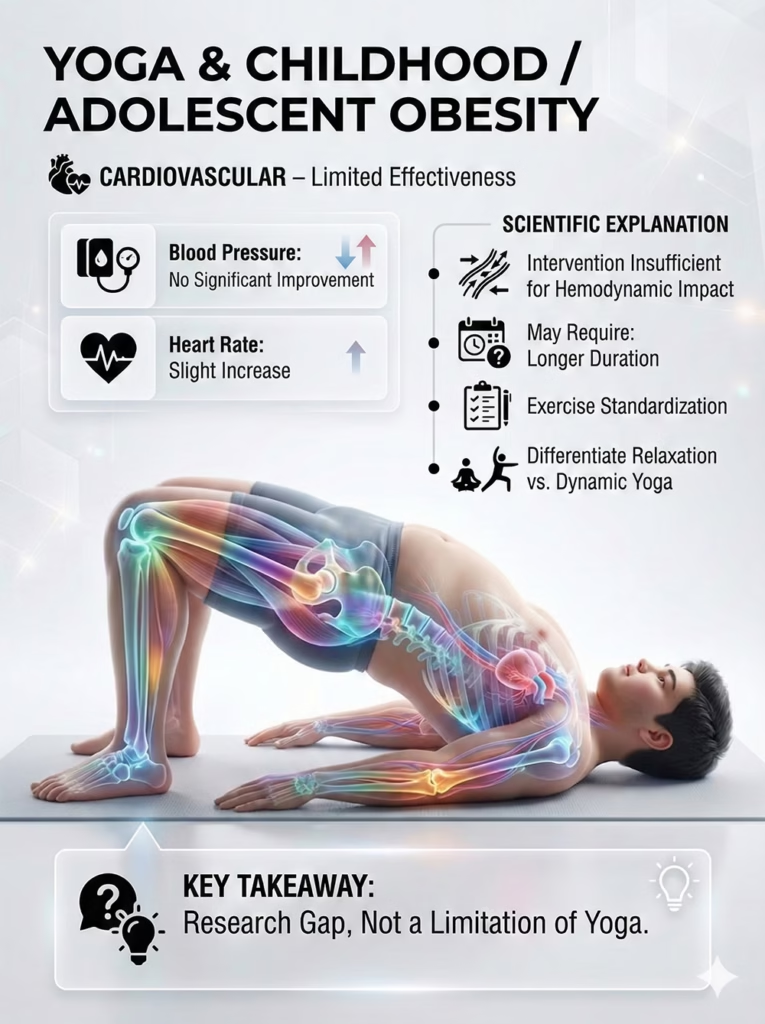
4. Cardiovascular Outcomes: Limited Evidence
The analysis indicated that Yoga did not yield clear improvements in blood pressure, and heart rate showed a slight, non-significant increase.
- Implication: Current Yoga interventions may not be of sufficient intensity or duration to significantly alter hemodynamics. Alternatively, longer duration or standardized protocols distinguishing between Restorative vs. Vinyasa styles are needed to elicit cardiovascular remodeling.
- This represents a research gap, necessitating further investigation, rather than a definitive flaw in the practice itself.
Part 5. Discussion
Why does a low-impact modality like Yoga effectively reduce fat in children? This section explores potential explanations for the observed fat reduction through a mind–body framework.
Mechanism: Beyond Caloric Expenditure
Unlike adult obesity, pediatric obesity is heavily influenced by emotional dysregulation and hormonal fluctuations.
- Stress Reduction Mechanism (Cortisol Modulation): Obese children often face significant psychological distress (e.g., body shaming, academic pressure). Chronic stress elevates Cortisol—a glucocorticoid that promotes visceral fat storage. Yoga reduces sympathetic tone and lowers Cortisol levels, potentially mitigating stress-related fat accumulation pathways
- Metabolic Mechanism: Yoga postures function as weight-bearing exercises. Although performed slowly, holding postures stimulates isometric muscle contraction, which builds lean muscle mass. Increased muscle mass elevates the Basal Metabolic Rate (BMR), allowing the child to oxidize energy more efficiently even at rest.
- Cognitive Mechanism (Mindfulness): Yoga enhances interoception (the ability to listen to internal bodily signals). This heightened awareness helps children control emotional eating—a primary behavioral driver of pediatric obesity.

Study Limitations
To maintain scientific objectivity, we must acknowledge the following limitations:
- Sample Size: Only 9 studies were included in the meta-analysis, which is a modest number for drawing broad generalizations.
- Heterogeneity: The variations in Yoga styles (Hatha, Vinyasa, etc.) and intervention duration across studies make it difficult to establish a single, standardized “dose-response” protocol.
Clinical Application (Pediatrician’s Perspective)
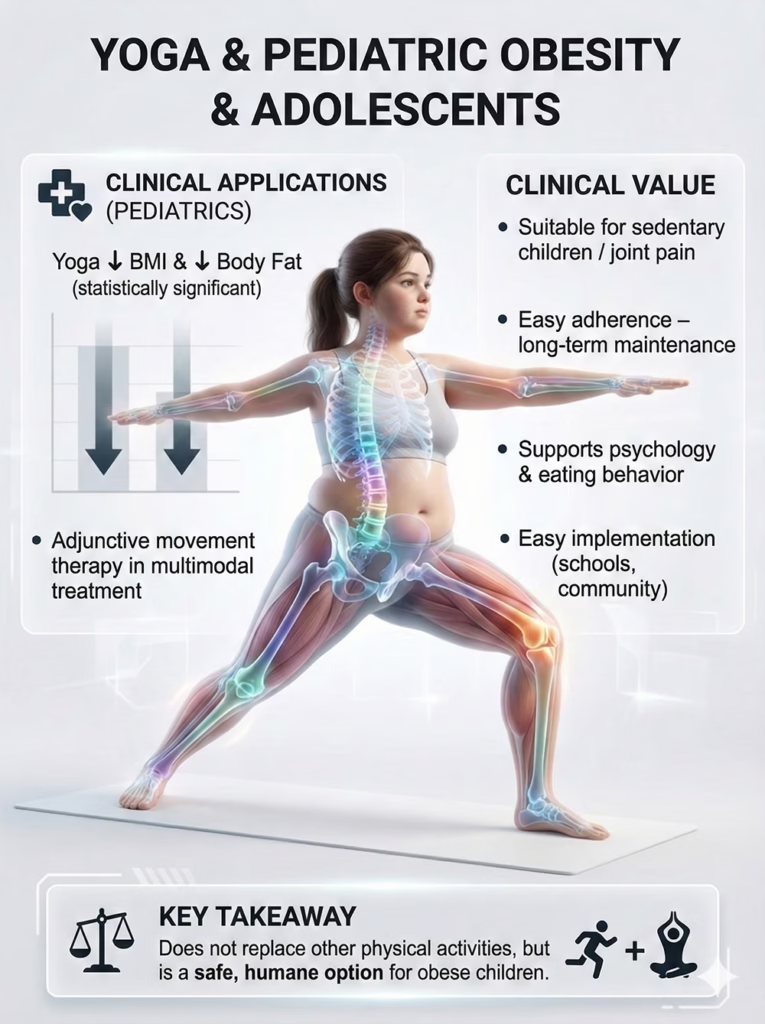
The meta-analysis demonstrates statistically significant improvements in BMI and body fat percentage. This opens a safe, feasible, and compliant intervention pathway in daily pediatric practice.
From a clinical standpoint, Yoga should be viewed as an adjunct therapy within a multimodal treatment plan (alongside nutritional counseling and behavioral therapy).
Practical Value for Pediatricians:
- Suitable for Sedentary/Comorbid Patients: Obese children often suffer from knee/ankle pain or reduced cardiorespiratory endurance, making high-impact cardio difficult. Low-to-moderate intensity Yoga avoids musculoskeletal overload.
- High Adherence: Yoga is highly personalized and non-competitive, helping children maintain long-term physical activity habits without the pressure of team sports.
- Psychological Benefits: It addresses anxiety and body image issues, indirectly supporting lifestyle and dietary compliance.
- Scalability: It is easy to integrate into school health systems or community clinics with minimal equipment.
Core Clinical Message: Yoga does not replace other forms of exercise, but it is a rational and patient-centered option, especially for children unsuitable for high-intensity regimens.
Application in Yoga Practice (Pediatric Yoga Coach’s Perspective)
This study provides a solid scientific basis for designing classes specifically targeted at overweight children.
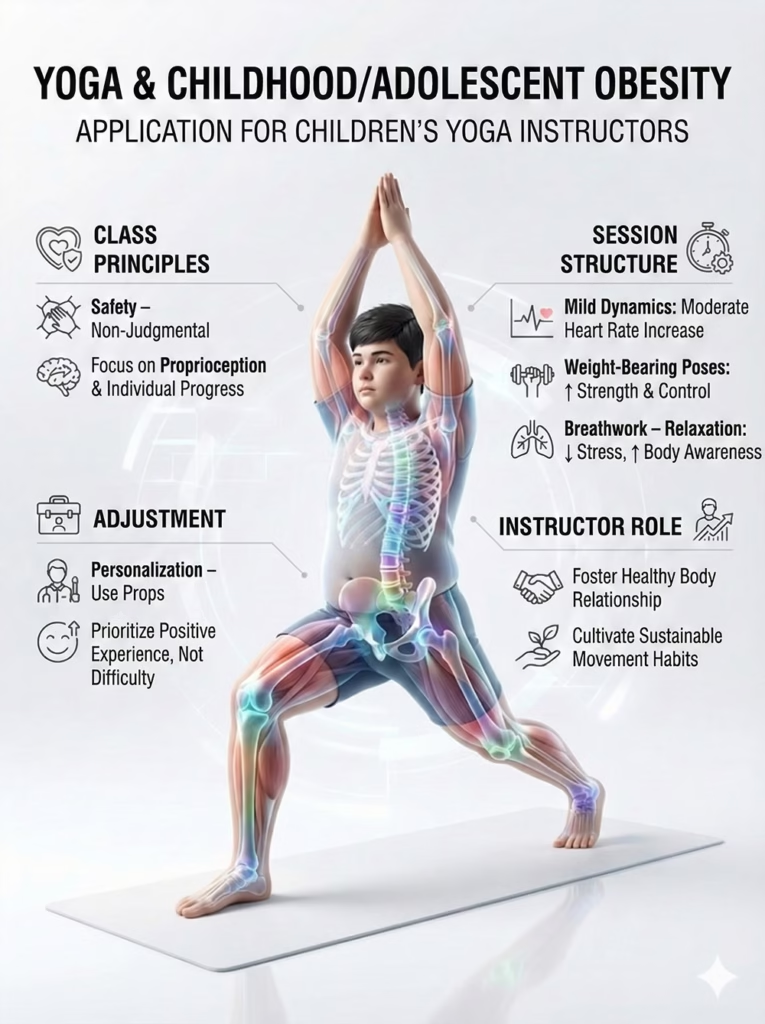
Design Principles:
- Safe & Non-judgmental Environment: Avoid appearance-based language. Focus on body functionality and personal progress.
- Dynamic-Static Balance:
- Gentle Flows: To moderately increase heart rate.
- Balancing/Holding Poses: To build strength and postural stability.
- Relaxation/Pranayama: To regulate emotions and stress response.
- Modifications: Use props (blocks, chairs) liberally. Prioritize a positive movement experience over pose difficulty or depth.
- Role of the Coach: Facilitate a healthy relationship with the body, serving as a guide for holistic well-being rather than just an instructor of movement.
Example of a Simple Class Sequence (45–60 minutes)
A practical structure may include:
- Warm-up (5–8 minutes):
- Strength & Stability Phase (15–20 minutes):
- Gentle Flow (8–10 minutes):
- Regulation & Relaxation (8–12 minutes):

This structure supports muscular engagement, moderate cardiovascular stimulation, and autonomic regulation while remaining joint-safe and psychologically supportive.
Childhood obesity significantly increases the risk of developing hypertension later in life. Our medical and yogic approach to hypertension explores long-term cardiovascular implications.
Part 6. Conclusion
The study by Caner and Yüce (2025) in Obesity Reviews provides moderate-to-high level evidence demonstrating a statistically significant, though modest, reduction in BMI and body fat percentage in obese children and adolescents.
This represents a potentially safe and supportive complementary intervention, offering a safe weight management pathway for the developing musculoskeletal system while potentially addressing psychological factors associated with pediatric obesity. Yoga warrants broad integration into school health programs and clinical treatment protocols for the younger generation.
References:
Caner, N., & Yüce, G. E. (2025). The Impact of Yoga Practices on Body Composition and Vital Signs in Children and Adolescents With Obesity: A Systematic Review and Meta-Analysis. Obesity Reviews. PMID: 40390197. PMCID: PMC12404879. DOI: 10.1111/obr.13947.
![The Biomechanical Demands of Standing Yoga Poses in Seniors [RESEARCH DECODED]](https://yogaismylife.vn/en/wp-content/uploads/2026/02/tu-the-chien-binh-cho-nguoi-cao-tuoi.webp)
![Effects of Yoga in People with Parkinson’s Disease [RESEARCH DECODED]](https://yogaismylife.vn/en/wp-content/uploads/2026/02/effects-of-yoga-in-parkinsons-disease-research-decoded.avif)

