Part 1. Introduction
Chronic non-specific low back pain (CLBP) is one of the most significant and persistent global health challenges. It is a multidimensional condition affecting physical function, work capacity, psychological well-being, and quality of life, from work capacity and social participation to mental health and sleep quality.
The economic burden caused by CLBP is immense, encompassing both direct healthcare costs and indirect costs due to lost productivity. Despite a myriad of treatment options – ranging from self-care and over-the-counter medications to physical therapy and invasive interventions – no single intervention has demonstrated consistent superiority across all patient populations.
In this context, clinical practice guidelines increasingly emphasize exercise therapy as a cornerstone intervention for CLBP. However, the question of “which exercise is best?” remains a subject of debate.
Movement is not just physical; it involves psychological factors such as beliefs, fear, and motivation. This has paved the way for growing interest in mind-body interventions.
Yoga, an ancient practice combining physical postures (asanas), breath control (pranayama), and meditation, has emerged as a popular choice. While countless individuals report benefits, and individual Randomized Controlled Trials (RCTs) offer support, a global clinical recommendation requires the highest level of evidence synthesis. This is the mission of a Cochrane Systematic Review.
Study Overview
- Title: Yoga for chronic non-specific low back pain
- Authors: Wieland LS, Skoetz N, Pilkington K, Vempati R, D’Adamo CR, Berman BM. (Cochrane Back and Neck Group)
- Publication Year: 2022 (Updated)
- Source: Cochrane Database of Systematic Reviews
- DOI: 10.1002/14651858.CD010671.pub3

Rationale for Selection and Significance
This work is considered the “gold standard” of evidence for several reasons:
- Cochrane Methodology: Cochrane is a global non-profit renowned for rigorous, transparent, and unbiased systematic reviews. Cochrane reviews are widely regarded as among the most rigorous sources in Evidence-Based Medicine (EBM).
- GRADE System: Beyond statistical results, Cochrane uses the GRADE system to assess the certainty of evidence (High, Moderate, Low, Very Low). This provides scientific honesty, telling us exactly how much we can trust the findings.
- Comprehensive Search: This review covers literature up to August 2021, without language restrictions.
- Clear Comparisons: It distinctly analyzes Yoga vs. Non-exercise, Yoga vs. Other Exercises, and Yoga as adjunctive therapy.
- Patient-Centered Outcomes: It focuses on what matters to patients: function, pain, quality of life, and safety.
Part 2. Objectives and Questions
Primary Objectives
The primary objective was to evaluate the benefits and harms of Yoga for treating chronic non-specific low back pain in adults compared to various control conditions (sham yoga, no treatment, minimal intervention, or other active treatments).
Review Questions
Instead of a single hypothesis, the review poses neutral research questions:
- Compared to no intervention or minimal intervention, is Yoga more effective for improving pain, function, and quality of life? Is it safe?
- Compared to other forms of exercise or active interventions, is Yoga superior, equivalent, or inferior?
- Does adding Yoga to another intervention provide synergistic benefits?
Part 3. Methodology
Design and Standards
This is a Systematic Review and Meta-analysis of RCTs, strictly adhering to the Cochrane Handbook and PRISMA reporting standards.
Participants and Inclusion Criteria
- Data Sources: A comprehensive search of major databases (CENTRAL, MEDLINE, Embase, etc.) and clinical trial registries up to August 31, 2021.
- Participants: 21 RCTs met the criteria, involving 2,223 participants. Most were women aged 40–50, recruited from both clinical and community settings across multiple countries (USA, India, UK, etc.).
- Risk of Bias (RoB): All 21 trials were assessed as having high risk of bias regarding “performance bias” (participants/instructors cannot be blinded in yoga) and “detection bias” (outcomes are self-reported). This is the primary reason the certainty of evidence was downgraded in the GRADE assessment.

Yoga Intervention and Comparisons
- Interventions: Programs mainly utilized Iyengar, Hatha, or Viniyoga styles. Most lasted 6–12 weeks, with 1–2 supervised sessions per week.
- Control Groups:
- Non-exercise controls: Usual care, education, or waitlist (10 trials).
- Back-focused exercise: Physical therapy or back strengthening (5 trials).
- Mixed controls: Compared Yoga against both types (4 trials).
- Mind-Body control: Yoga vs. Qigong (1 trial).
- Yoga + Exercise: (1 trial).
- Note: No studies used “Sham Yoga” (placebo).

Measures and Analysis
- Major Outcomes: Back-specific function (e.g., Roland-Morris Disability Questionnaire – RMDQ), Pain intensity, Clinical improvement, Quality of Life (QoL), Depression, and Adverse events.
- Statistical Analysis: Used Mean Difference (MD) or Standardized Mean Difference (SMD) for continuous data; Risk Ratio (RR) for binary data.
- MCID (Minimal Clinically Important Difference): Pre-defined thresholds for “meaningful” change were 5 points for RMDQ (0-24 scale) and 15 points for Pain (0-100 scale).

Part 4. Results
The results are presented with nuance, distinguishing between statistical significance and clinical importance.
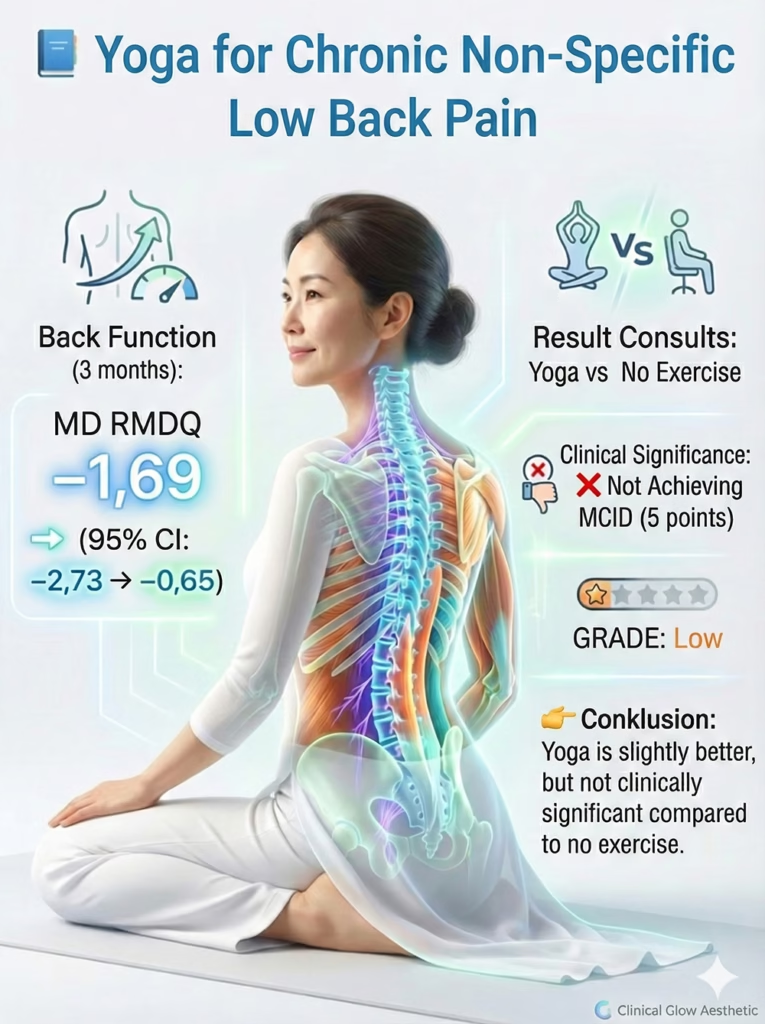
Comparison 1: Yoga vs. Non-Exercise Controls
Does Yoga work better than doing nothing or usual care?
Back-specific Function (3 months):
- Result: Small improvement. MD = -1.69 (95% CI: -2.73 to -0.65).
- Clinical Significance: Unimportant. This means that although the numbers changed, most patients would likely not perceive a meaningful functional improvement.
- Certainty (GRADE): Low.
Pain Intensity (3 months):
- Result: Small reduction. MD = -4.53 (scale 0-100) (95% CI: -6.61 to -2.46).
- Clinical Significance: Unimportant. Falls well below the MCID threshold of 15 points.
- Certainty (GRADE): Moderate.

Clinical Improvement:
- Result: Yoga participants were 2.33 times more likely to report overall improvement (RR = 2.33).
- Certainty: Low.

Adverse Events:
- Result: Yoga increased the risk of adverse events (mostly temporary back pain) compared to non-exercise (RR = 4.76). However, most events were mild and transient.
- Certainty: Low.

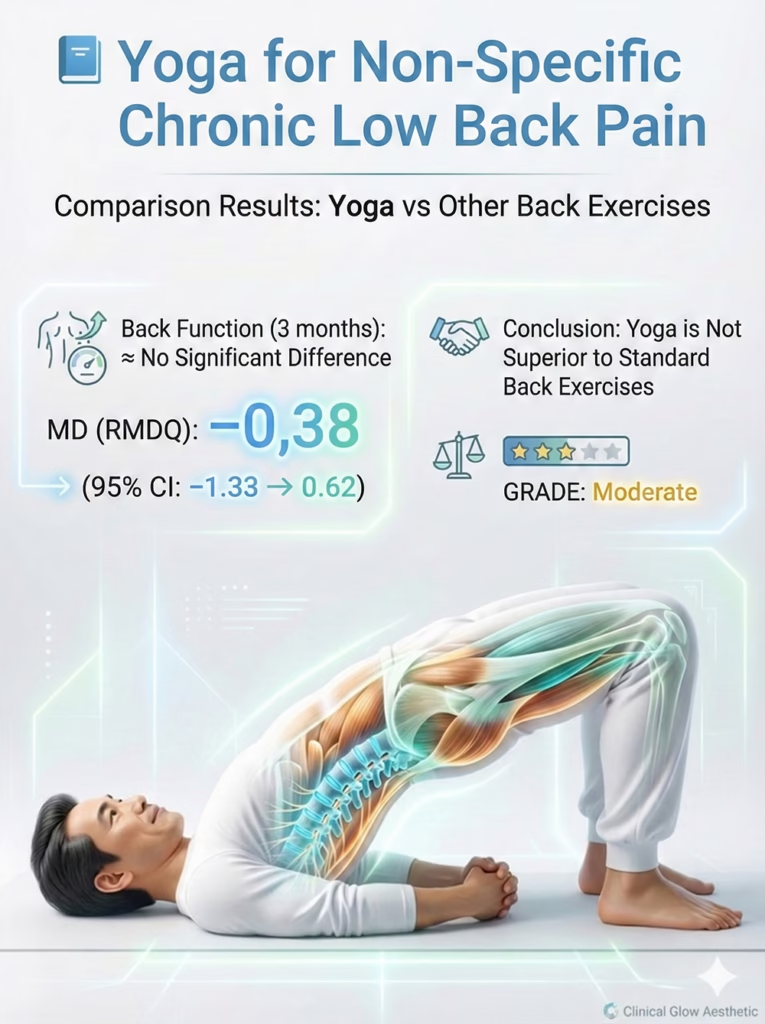
Comparison 2: Yoga vs. Back-Focused Exercise Controls
Is Yoga better than physical therapy or other back exercises?
Back-specific Function (3 months):
- Result: Little to no difference (MD = -0.38; 95% CI: -1.33 to 0.62).
- Certainty: Moderate.
Pain Intensity (3 months):
- Result: Little to no difference (MD = 2.68; 95% CI: -2.01 to 7.36).
- Certainty: Very Low.
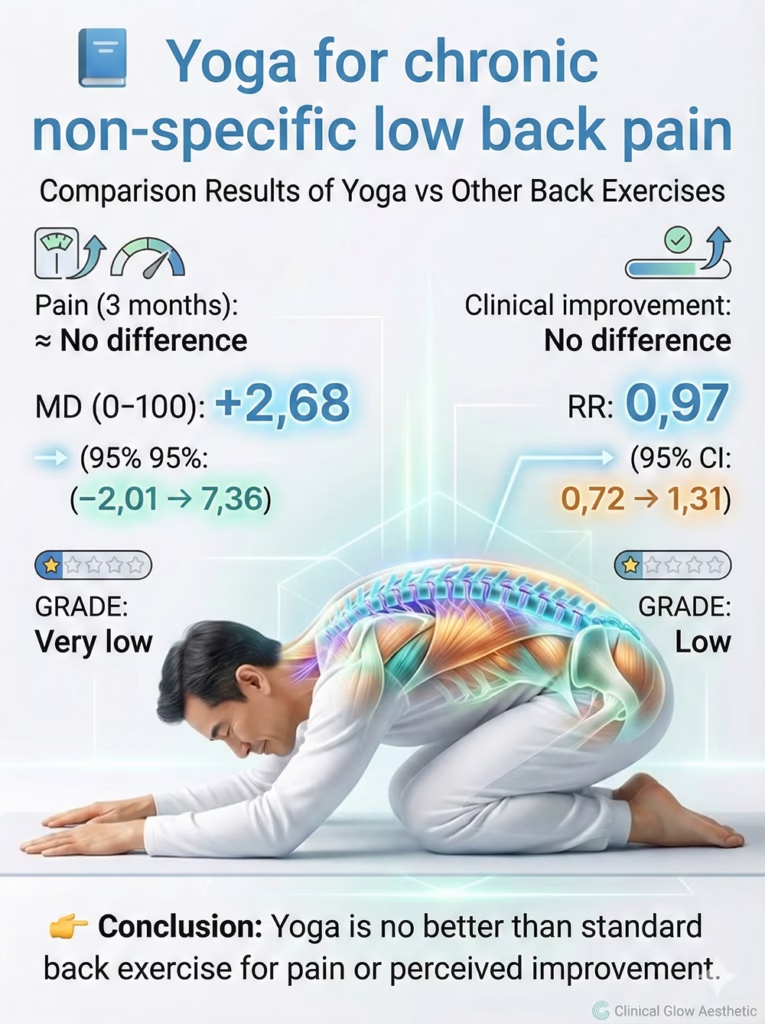
Adverse Events:
- Result: No significant difference in risk between Yoga and other exercises (RR = 0.93).
- Certainty: Low.
Summary of Findings
- Yoga > Doing Nothing (Slightly): Yoga is better than non-exercise, but the effect size for pain and function is small and arguably not clinically “transformative” for the average patient, though some individuals may benefit significantly.
- Yoga ~ Other Exercises: There is no reliable evidence that Yoga is superior to other active back-focused exercises.
- Quality of Evidence: Generally Low to Moderate, primarily due to the inability to blind participants (risk of bias).
- Safety: Yoga has a higher risk of minor side effects (temporary pain) compared to resting, but is as safe as other exercises.

Part 5. Discussion
This Cochrane review paints a realistic and humble picture of Yoga’s role in CLBP treatment.
Mechanism: Why “Small” Improvements?
Even if the effect size is small, While the review did not directly assess mechanisms, plausible pathways may include:
- Physical Movement: Even gentle asanas stimulate the musculoskeletal system, maintain range of motion, and activate core stabilizers.
- Breath (Pranayama): Slow breathing regulates the Autonomic Nervous System, reducing sympathetic (stress) activity, which may desensitize pain pathways.
- Mindfulness & Interoception: Yoga changes the relationship with pain. Instead of fear-avoidance or catastrophizing, patients learn to observe sensations. This reduces the “suffering” component of pain, even if the “sensation” intensity drops only slightly.
These findings are consistent with a bottom-up regulatory pathway, where yoga may influence pain perception through autonomic nervous system modulation rather than direct cognitive enhancement — a mechanism further explored in our analysis on nervous system rebalancing and stress physiology.

Why is Yoga not superior to other exercises?
The “Common Active Ingredients” hypothesis: The review suggests that for pain and function, the specific “mind-body” elements of Yoga do not add a measurable advantage over standard exercise. Both Yoga and Physical Therapy share core therapeutic factors:
- Active movement (reversing deconditioning).
- Strengthening and flexibility.
- Professional supervision.
- Building confidence/reducing fear of movement.
Understanding GRADE Ratings
A “Low Certainty” rating does not mean Yoga is ineffective. It reflects scientific honesty: due to study limitations (lack of blinding), we cannot be absolutely certain of the exact size of the benefit. Future research could change these estimates.
Medical Application (Doctor’s Perspective)
- Recommendation: Doctors can present Yoga as a safe, evidence-based option that offers small improvements in function and pain compared to inactivity.
- Patient Preference is Key: Since Yoga and other exercises have similar efficacy, the best choice is what the patient enjoys and will stick with.
- Risk Counseling: Inform patients that temporary increases in back pain are possible (similar to starting a gym routine) but generally safe.
Similar systemic regulatory effects have also been observed in cardiovascular contexts, as discussed in our breakdown of yoga’s role in blood pressure and autonomic regulation.

Yoga Practice Application (Instructor’s Perspective)
- Calibrate Expectations: Yoga is not a corrective “fix” for chronic low back pain. Instructors should frame it as a structured movement approach that may produce modest functional gains over time rather than dramatic pain elimination.
- Dose & Progression Matter: Given the elevated risk of transient symptom flare-ups, careful sequencing, gradual load progression, and individualized modifications are essential. Therapeutic intent must outweigh aesthetic form.
- Movement Over Modality: Evidence shows Yoga performs similarly to other back-focused exercises. The priority is sustainable movement adherence. If a student prefers swimming, walking, or physical therapy, that is equally valid. Consistency drives outcomes.

While this randomized trial demonstrates that yoga significantly improves pain intensity and functional disability in chronic non-specific low back pain, sustainable recovery requires more than statistical significance. It demands a structured integration of biomechanics, neuromuscular retraining, and nervous system regulation. For a deeper clinical framework that translates evidence into step-by-step therapeutic application, explore our guide on a medical and yogic roadmap for chronic low back pain rehabilitation.
Part 6. Conclusion
This Cochrane Systematic Review provides the most rigorous objective assessment of Yoga for CLBP to date. The conclusions are cautious:
- Low-to-moderate certainty evidence suggests Yoga provides small short-term improvements in back-related function and pain compared to non-exercise controls, though these effects may fall below clinically meaningful thresholds.There is very low-to-moderate certainty evidence that there is little to no difference between Yoga and other back-focused exercises.
- Yoga carries a higher risk of minor adverse events (increased back pain) than non-exercise but is comparable to other exercises.
In summary: Yoga is a safe and reasonable therapeutic option, but it is not a superior “magic bullet.” Its greatest value lies in providing an additional evidence-based choice, allowing treatment to be personalized based on patient preference.
References
- Wieland, L. S., Skoetz, N., Pilkington, K., et al. (2022). Yoga for chronic non-specific low back pain. Cochrane Database of Systematic Reviews, Issue 11. Art. No.: CD010671.
- Higgins, J. P., et al. (2011). The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ, 343.
- Guyatt, G. H., et al. (2008). GRADE: an emerging consensus on rating quality of evidence. BMJ, 336(7650).
![The Biomechanical Demands of Standing Yoga Poses in Seniors [RESEARCH DECODED]](https://yogaismylife.vn/en/wp-content/uploads/2026/02/tu-the-chien-binh-cho-nguoi-cao-tuoi.webp)
![The Impact of Yoga on Pediatric Obesity [RESEARCH DECODED]](https://yogaismylife.vn/en/wp-content/uploads/2026/02/The-Impact-of-Yoga-on-Pediatric-Obesity.avif)

