Part 1: Introduction
Sleep disorders, particularly insomnia, place a disproportionate burden on women, who face a 1.41 times higher risk than men due to complex hormonal fluctuations across life stages (pregnancy, menopause). Chronic sleep deprivation severely impairs daily functioning and exponentially increases mental health, cardiovascular, and metabolic risks.
Currently, Cognitive Behavioral Therapy for Insomnia (CBT-I) is the “gold standard” but suffers from high costs and low accessibility. Consequently, hypnotics (sleep medications) remain the default, despite concerning side effects like dependency, daytime somnolence, and cognitive impairment.
This highlights the urgent need for safe, accessible complementary interventions. Yoga—integrating physical postures (Asana), breathwork (Pranayama), and meditation (Dhyana)—has emerged as a potent mind-body solution. It theoretically modulates sleep by:
- Autonomic Regulation: Shifting the nervous system from a sympathetic “fight-or-flight” state to parasympathetic “rest-and-digest,” directly mitigating insomnia’s hyperarousal.
- Stress Reduction: Disarming psychological stress, a primary trigger and sustainer of sleep disruption.
- Endocrine Modulation: Elevating endogenous melatonin (sleep hormone) while reducing cortisol (stress hormone).
While individual trials show promise, high-level synthesized evidence is crucial to validate Yoga’s efficacy specifically for women.
Insomnia in women is frequently associated with chronic sympathetic overactivation and impaired parasympathetic recovery. Rather than treating sleep as an isolated symptom, it is often more effective to address the underlying autonomic imbalance through structured nervous system regulation strategies.
Study Overview
- Title: The effect of yoga on sleep quality and insomnia in women with sleep problems: A systematic review and meta-analysis
- Authors: Wang, W.L., et al.
- Year: 2020
- Journal: BMC Psychiatry
- Link (PMC): https://pmc.ncbi.nlm.nih.gov/articles/PMC7193366/
- DOI: 10.1186/s12888-020-02566-4
Why This Study Matters
Wang et al.’s research is a large-scale, highly valuable meta-analysis. It pools data from 19 RCTs involving over 1,800 female participants. More importantly, it does not offer a simplistic “yes or no” answer. Instead, it reveals a crucial scientific nuance: the distinct difference between Yoga’s impact on subjective sleep quality (PSQI) versus the clinical severity of insomnia (ISI). Furthermore, its subgroup analyses (e.g., breast cancer patients, menopausal women) provide profound, context-specific insights into where Yoga is most effective.
Part 2: Objectives and Hypotheses
Primary Objective
To systematically evaluate the efficacy and safety of Yoga interventions for sleep problems in women, based exclusively on evidence from Randomized Controlled Trials (RCTs).
Scientific Hypothesis
Based on Yoga’s established neuro-modulatory and stress-reducing effects, researchers hypothesized that pooled data would demonstrate a statistically significant superiority of Yoga interventions in improving sleep metrics (quality and severity) compared to control groups (e.g., waitlist, usual care, or non-exercise education).
Part 3: Methodology
Study Design
A systematic review and meta-analysis of Randomized Controlled Trials (RCTs).
Participants and Inclusion Criteria
- Data Sources: A comprehensive search of 6 major medical databases (Medline/PubMed, ClinicalKey, ScienceDirect, Embase, PsycINFO, and Cochrane Library) up to June 2019.
- Participants: Post-screening, 19 RCTs were included, comprising 1,832 female patients (aged ≥18) reporting sleep disturbances.
- Inclusion Criteria: RCTs comparing a Yoga intervention to a control group (usual care, waitlist, or education) in women with sleep problems.
The Yoga Intervention
Interventions varied widely, encompassing styles such as Iyengar, Hatha, Tibetan, and Restorative Yoga. Most protocols integrated postures (Asana), breathwork (Pranayama), and relaxation/meditation. Intervention duration ranged from 1 to 24 weeks.

Clinical Outcome Measures Primary outcomes were measured using standardized subjective tools. Data was synthesized using Standardized Mean Differences (SMD).
- Sleep Quality: Primarily measured by the Pittsburgh Sleep Quality Index (PSQI). A 19-item self-report scale assessing 7 components (subjective quality, latency, duration, efficiency, disturbances, medication use, and daytime dysfunction). Higher scores indicate poorer sleep.
- Insomnia Severity: Measured by the Insomnia Severity Index (ISI). A 7-item scale assessing the patient’s perception of difficulty initiating/maintaining sleep, early waking, sleep satisfaction, and daytime impairment. Higher scores indicate greater severity.
- Objective Measures: A minority of studies used Polysomnography (PSG) or actigraphy, but data was insufficient for robust meta-analysis.
- Safety: Incidence of serious adverse events was recorded.
Part 4: Results
The meta-analysis of 19 RCTs involving 1,832 women yielded highly nuanced results, exposing a critical scientific paradox regarding how Yoga impacts sleep.
Overall Meta-Analysis
When pooling data from all 19 studies, Yoga demonstrated a statistically significant overall positive effect in improving general sleep problems (SMD = -0.327; 95% CI: -0.506 to -0.148; P < 0.001). This is considered a small-to-medium effect size.
However, breaking down the specific scales and patient subgroups reveals a much more complex picture.
The POSITIVE Findings (Statistically Significant)
- Subjective Sleep Quality (PSQI Scale): Analyzing 16 RCTs that used the PSQI, the Yoga group showed a highly significant improvement in sleep quality (SMD = -0.54; P = 0.003).
- Clinical Significance: An SMD of -0.54 represents a “medium” effect size. This means the improvement is not just a statistical number; it is a palpable change felt by the patient. The PSQI measures broad factors, including subjective satisfaction and daytime dysfunction. This suggests Yoga effectively helps women feel their sleep is better and less disruptive to their daily lives.
The “NEGATIVE” Findings (Not Statistically Significant) – The Scientific Paradox
This is the study’s most crucial revelation. While Yoga improved “sleep quality” (PSQI), it failed to improve the “core” metrics of clinical insomnia and showed no efficacy in high-risk physiological subgroups.
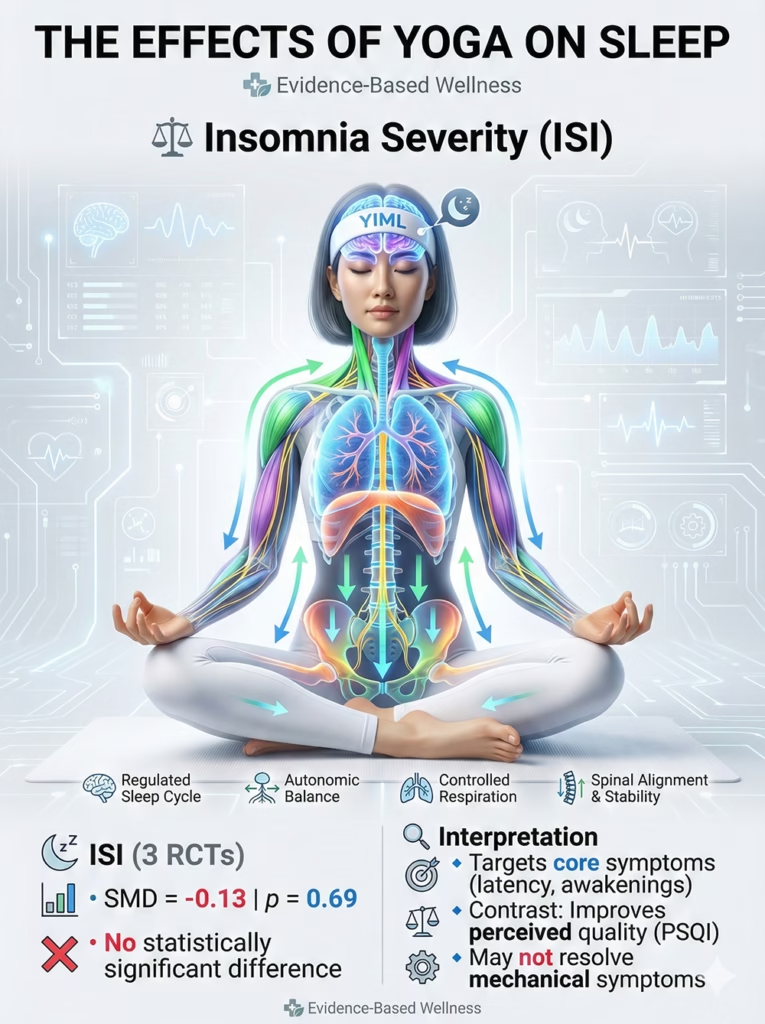
- Insomnia Severity (ISI Scale): Analyzing 3 RCTs using the ISI, there was no statistically significant difference between Yoga and control groups (SMD = -0.13; P = 0.69).
- Significance: The ISI specifically measures core clinical symptoms: sleep latency (time to fall asleep) and nocturnal awakenings. Yoga’s failure here, contrasted with its success on the PSQI, creates a paradox: Yoga appears to make people more “satisfied” with their rest, but it may not actually cure the mechanical symptoms of clinical insomnia.
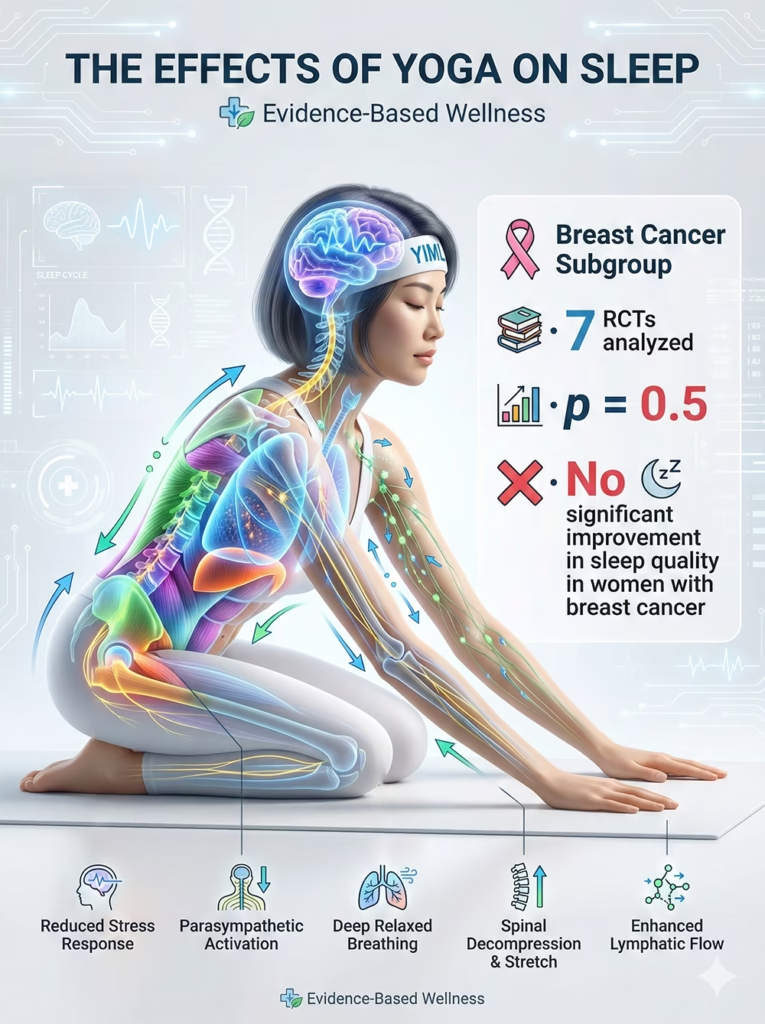
- Breast Cancer Subgroup: Across 7 RCTs, Yoga showed no efficacy in improving sleep quality for women with breast cancer (P = 0.5).
- Peri/Post-Menopausal Subgroup: Across 4 RCTs, Yoga similarly showed no statistically significant efficacy for this demographic (P = 0.34).

Safety Profile Yoga was consistently reported as safe, with no serious adverse events linked to the interventions across the included studies.
Part 5: Discussion
The results of this meta-analysis move beyond a simplistic “Yoga is good for sleep” narrative. It presents a nuanced puzzle: Why does Yoga improve general “sleep quality” (PSQI) but fail to resolve clinical “insomnia” (ISI) and falter in menopausal and oncology patients?
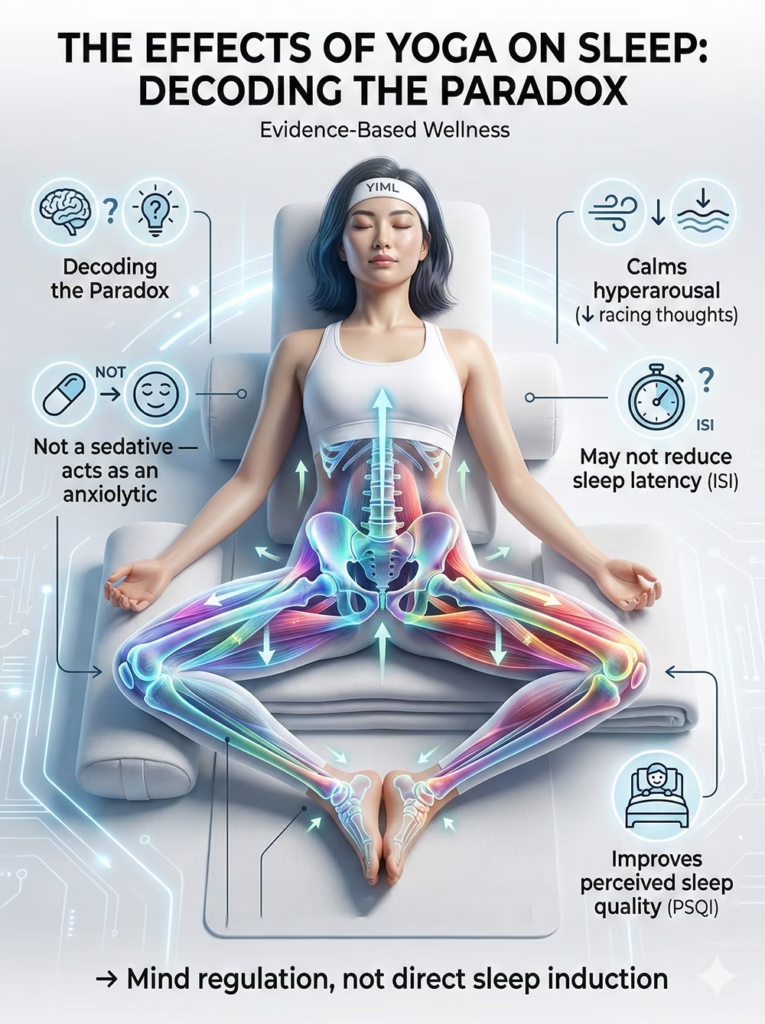
Decoding the Paradox: “Quality” (PSQI) vs. “Insomnia” (ISI)
This central finding suggests that Yoga’s primary mechanism is not acting as a physiological “sedative” (like a sleeping pill), but rather as an “anxiolytic” (anxiety reducer) and emotional regulator.
- The Mechanism: Practices like Pranayama (breathwork) and meditation calm the sympathetic nervous system and reduce the hyperarousal (racing thoughts) experienced by insomniacs.
- The Clinical Reality: Yoga may not significantly reduce the actual minutes it takes to fall asleep (what the ISI measures). Instead, it reduces the patient’s anxiety, frustration, and “fight” against wakefulness. Patients learn to accept and relax even while awake. This profound shift in the psychological relationship with sleep reflects as improved PSQI scores. Yoga acts as “mind regulation” rather than direct “sleep treatment.”
Before initiating any therapeutic yoga protocol for insomnia, individuals should complete a structured pre-participation screening to identify cardiovascular, musculoskeletal, or neurological risk factors.
Explaining the “Negative” Results in Menopause and Breast Cancer
Why did this mind-body intervention fail the groups that seemingly need it most?
- Overwhelming Biological Drivers: Unlike primary insomnia (often driven by stress), insomnia in menopausal and oncology patients has overwhelming biological and pharmacological drivers that Yoga (at studied doses) cannot override.
- Menopause: Insomnia is directly triggered by hot flashes and night sweats—a profound neuroendocrine disruption due to estrogen withdrawal, not merely psychological stress.
- Breast Cancer: Sleep is devastated by physical pain, neurotoxic side effects of chemo/radiation, circadian disruption, and severe existential distress.
Chronic sleep disturbance is often accompanied by sustained stress activation, which may gradually influence cardiovascular regulation and blood pressure patterns. This highlights the importance of an integrated yoga therapy approach for hypertension management when designing sleep-focused therapeutic programs.
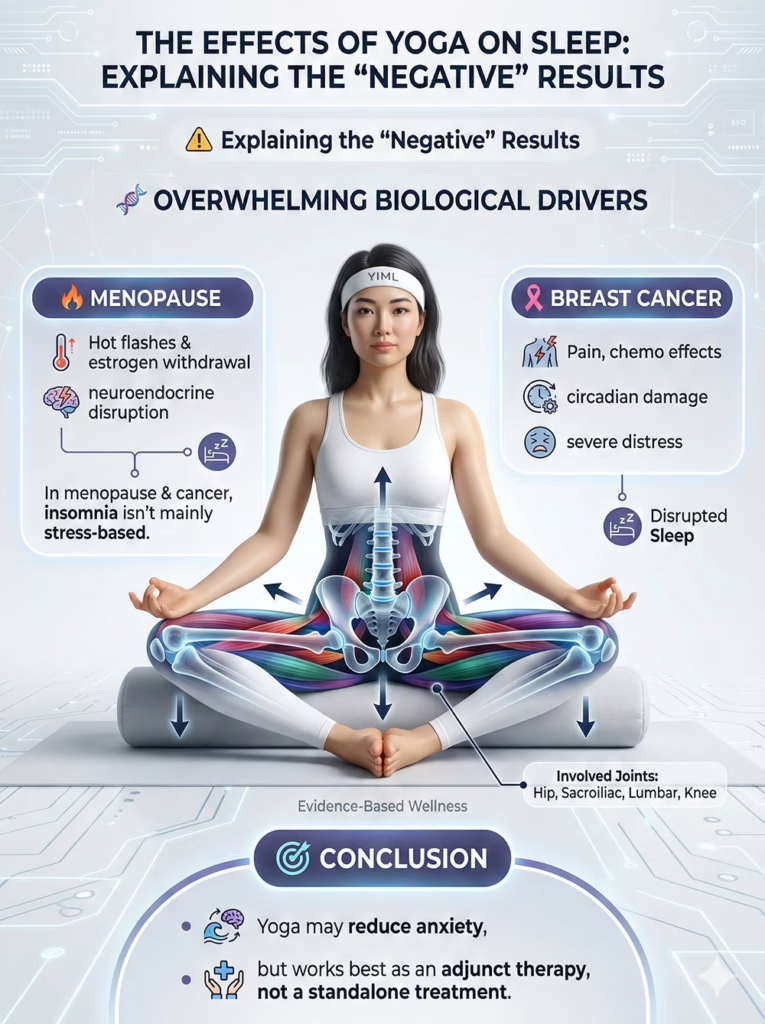
- Conclusion: Yoga can reduce baseline anxiety for these patients, but it is not potent enough to independently counteract hormonal hot flashes or cancer-related pain. In these complex secondary insomnias, Yoga must be strictly viewed as an adjunctive therapy alongside primary medical interventions (e.g., Hormone Replacement Therapy, pain management, or specialized CBT-I).
Study Limitations
- Methodological Quality: The authors noted low methodological quality in the original 19 RCTs, primarily regarding blinding (which is inherently impossible in behavioral interventions like Yoga).
- High Heterogeneity (I² = 58%): Expected, given the vast differences in Yoga styles, durations, and diverse patient populations.
- Subjective Reliance: Results relied heavily on self-reported scales (PSQI, ISI). Few studies used objective actigraphy or Polysomnography (PSG) to verify actual sleep time changes.
- Publication Bias: Funnel plot analysis indicated a potential bias (P = 0.05), suggesting positive trials are more likely to be published than negative ones.
Clinical Application (The Physician’s Perspective)
- First-Line Safe Tool: Physicians can confidently recommend Yoga as a safe, non-pharmacological intervention for “general” sleep disturbances in women, particularly those rooted in stress and anxiety.
- Expectation Management: It is vital to counsel patients: “Yoga will help you relax, reduce sleep anxiety, and improve your overall quality of life. However, it is not a ‘cure’ for clinical insomnia, especially if you are menopausal or undergoing cancer treatment. In those cases, it is an excellent supportive therapy alongside your medical treatment.”
Practical Application (The Yoga Therapist’s Perspective)
- Focus on “Regulation,” Not “Sedation”: When designing classes for insomnia, the goal isn’t to create postures that “force” sleep. The priority must be parasympathetic regulation via Pranayama, Yoga Nidra (deep relaxation), and meditation.
- Patient Education: Therapists must teach students that the goal is not to “fight” insomnia, but to train the mind to relax and surrender. Reducing the struggle is the therapy.
- Specialization is Required: The negative results in menopause and oncology highlight that a “one-size-fits-all” Yoga class is ineffective. Therapists need specialized training in the pathophysiology of these conditions to design safe, targeted restorative protocols.

These scientific insights demonstrate that Yoga regulates the entire nervous system rather than just inducing sleep. To translate this into practical application, explore our comprehensive therapeutic guide: A Roadmap to Pain Relief & Restorative Sleep
Part 6: Conclusion
The meta-analysis by Wang et al. (2020) provides a profoundly important perspective on Yoga’s role in women’s sleep health. The conclusion is not a binary “does it work?” but rather “how does it work, and for whom?”
The Dual Message:
- For general, stress-related sleep problems: Yoga is a moderately effective intervention that significantly improves subjective sleep quality (PSQI). Its primary mechanism is anxiolytic—reducing arousal and changing the patient’s psychological relationship with rest.
- For core insomnia symptoms (ISI) and populations with strong biological drivers (menopause, breast cancer): Yoga, according to current protocols, does not show standalone efficacy.
This finding does not diminish Yoga; it accurately positions it. Yoga is not a panacea or a universal “sleeping pill.” It is a powerful tool for neural retraining and managing the psychological burden of sleep disorders. Yoga teaches us how to “rest” even when we cannot “sleep”—and that may be its most profound therapeutic benefit.
References
- Wang, W. L., et al. (2020). The effect of yoga on sleep quality and insomnia in women with sleep problems: a systematic review and meta-analysis. BMC Psychiatry, 20(1), 195.
- Buysse, D. J., et al. (1989). The Pittsburgh Sleep Quality Index (PSQI): a new instrument for psychiatric practice and research. Psychiatry Research.
- Bastien, C. H., et al. (2001). Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Medicine.
- Zhang, B., & Wing, Y. K. (2006). Sex differences in insomnia: a meta-analysis. Sleep.
- Mitchell, T., & Tsuchida, R. (2018). Cognitive behavioral therapy for insomnia (CBT-I). Missouri Medicine.
![The Biomechanical Demands of Standing Yoga Poses in Seniors [RESEARCH DECODED]](https://yogaismylife.vn/en/wp-content/uploads/2026/02/tu-the-chien-binh-cho-nguoi-cao-tuoi.webp)
![The Impact of Yoga on Pediatric Obesity [RESEARCH DECODED]](https://yogaismylife.vn/en/wp-content/uploads/2026/02/The-Impact-of-Yoga-on-Pediatric-Obesity.avif)

