Part 1: Introduction
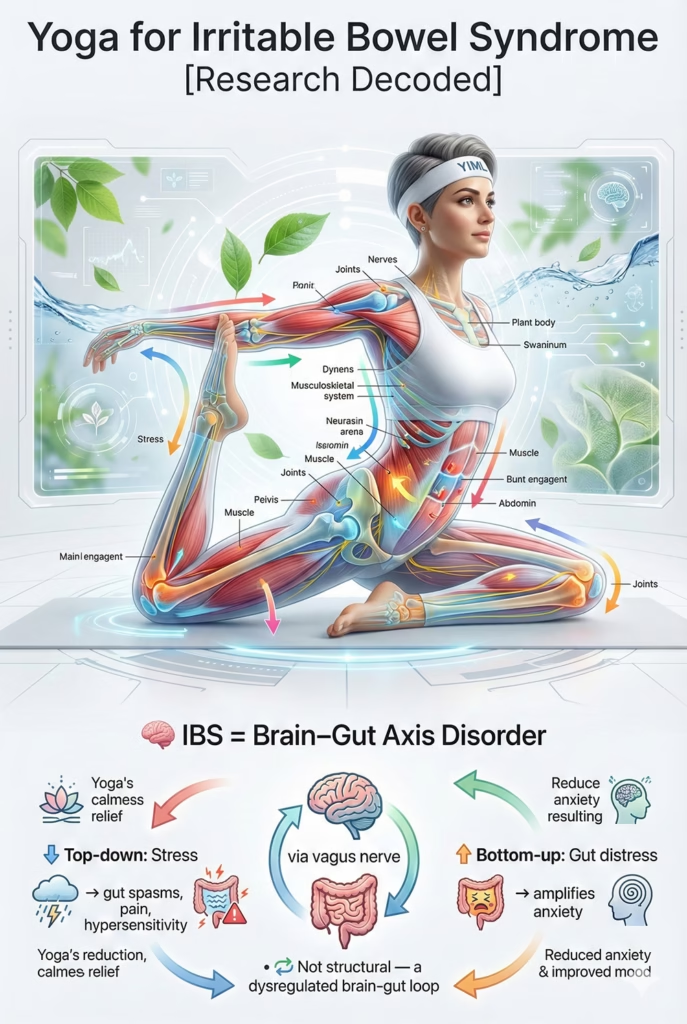
Irritable Bowel Syndrome (IBS) is not a structural disease, but a primary Disorder of the Brain-Gut Axis. Characterized by chronic abdominal pain, bloating, and erratic bowel habits, its pathogenesis is a bidirectional vicious cycle mediated by the Vagus Nerve:
- “Top-Down” Dysregulation: Chronic stress locks the brain in sympathetic overdrive, cascading signals that induce intestinal spasms, visceral hypersensitivity (pain), and hyperpermeability (“leaky gut”).
- “Bottom-Up” Dysregulation: Enteric abnormalities transmit somatic distress signals back to the brain, amplifying central anxiety.
The Therapeutic Gap Standard medical protocols are fragmented. GI-targeted treatments (antispasmodics, restrictive diets) only mask peripheral symptoms, while central neuromodulators (low-dose antidepressants) face high patient resistance. A comprehensive intervention modulating both targets simultaneously is critical.
Yoga: The “Theoretically Perfect” Intervention Yoga is theoretically well-positioned to modulate key components of the Brain-Gut Axis:
- Pranayama & Meditation: May enhance parasympathetic activity and vagal tone (Parasympathetic activation) to antagonize stress-induced sympathetic overdrive and soothe intestinal spasms.
- Asana: Gentle twists provide targeted visceral massage and deep abdominal relaxation.
- Mindfulness: Interrupts the pain-catastrophizing loop, decoupling physical sensation from psychological panic.
Despite this robust theoretical alignment, dozens of Randomized Controlled Trials (RCTs) have yielded notoriously inconsistent outcomes, leading to profound confusion within the medical community.
Study Overview
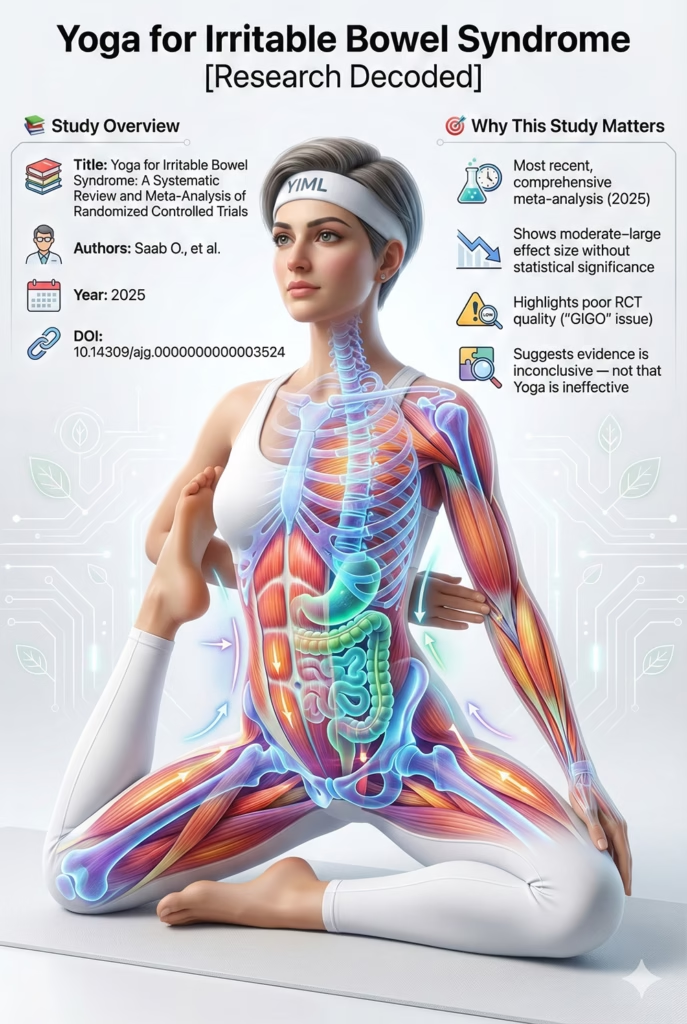
- Title: Yoga for Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
- Authors: Saab, O., et al.
- Published: 2025
- Link: https://pubmed.ncbi.nlm.nih.gov/40358469/
- DOI: 10.14309/ajg.0000000000003524
Why Analyze This Specific Study?
This 2025 paper by Saab et al. is the most recent and comprehensive meta-analysis on the subject. Its scientific value lies in its seemingly “negative finding,” which directly challenges the “theoretically perfect” status of Yoga for IBS. It presents a classic scientific paradox: How can an intervention demonstrate a moderate-to-large Effect Size (SMD), yet fail to achieve statistical significance? This study is a textbook illustration of the “Garbage In, Garbage Out” (GIGO) phenomenon in medical research. It does not prove that Yoga is “useless”; rather, it highlights that the existing RCTs on Yoga are of such low methodological quality that definitive conclusions are currently impossible to draw. Decoding this paradox is essential for understanding the future of Yoga research.
Part 2: Objectives and Hypotheses
Primary Objectives The authors conducted this systematic review and meta-analysis to:
- Synthesize Evidence: Pool data from all existing RCTs to evaluate Yoga’s overall efficacy on IBS symptoms.
- Resolve Inconsistencies: Address the conflicting findings present in earlier, smaller reviews.
- Comprehensive Evaluation: Quantify Yoga’s impact not only on GI symptoms but also on the core psychosocial drivers of the Brain-Gut Axis: Anxiety, Depression, and Quality of Life (QoL), domains that have shown mixed but promising results in prior analyses such as our breakdown of Yoga for depressive disorder.
The Scientific Hypothesis While not explicitly stated, the robust theoretical framework suggests the implicit hypothesis was: When pooling data from 11 RCTs, Yoga will demonstrate superior, statistically significant efficacy compared to control groups across all measured domains (GI symptoms, anxiety, depression, and QoL). (Spoiler: This hypothesis was rejected by their own pooled results).
Part 3: Methodology
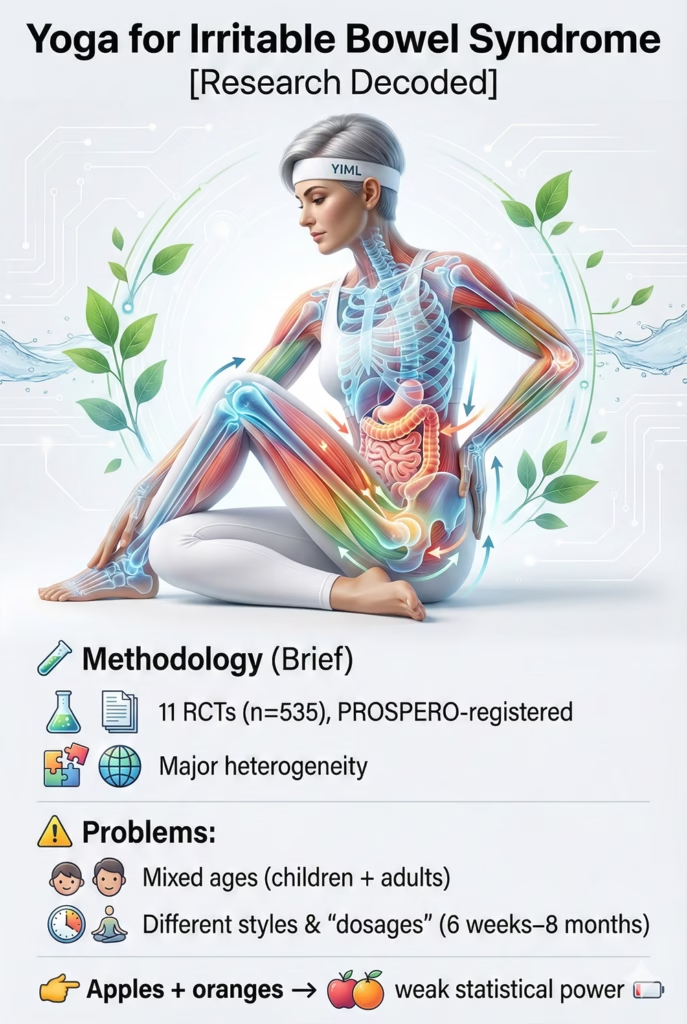
Study Design A Systematic Review and Meta-analysis of Randomized Controlled Trials (RCTs), pre-registered with PROSPERO to ensure methodological transparency.
Participants and Selection Criteria
- Search: A comprehensive search across 5 major databases (PubMed, EMBASE, WOS, SCOPUS, Cochrane) up to October 2024.
- Yield: 11 RCTs involving a total of 535 patients were included.
Analyzing the “Roots of the Paradox” (Methodological Flaws) The seeds of statistical failure are glaringly obvious within the methodology section. The authors reported massive, prohibitive heterogeneity (inconsistency) among the included trials:
1. Population Heterogeneity:
- 7 RCTs focused on adults.
- 3 RCTs focused on pediatric or adolescent patients.
- 1 RCT mixed adolescents and young adults.
- The Problem: Pooling data from a 10-year-old child and a 50-year-old adult is a major statistical flaw. The psychosocial drivers and neurodevelopmental status of the Brain-Gut Axis differ vastly between these groups.
2. Intervention Heterogeneity (“Dosing”):
- Yoga styles varied wildly across trials.
- Program duration ranged from 6 weeks to 8 months.
- Session duration ranged from 40 to 90 minutes.
- The Problem: This is comparing apples to oranges. A 6-week, 40-minute intervention cannot be statistically pooled with an 8-month, 90-minute intervention. They are entirely different “dosages” of therapy.
3. Control Group Heterogeneity (High Risk of Bias)
The authors explicitly noted a “high risk of bias,” implying that the control groups across these 11 RCTs were weak (e.g., “usual care” or waitlist) and lack of blinding was pervasive.
Methodological Conclusion: Before even examining the results, it is evident that these 11 RCTs represent a methodological mess. Attempting to pool them via meta-analysis inevitably generates massive Confidence Intervals, rendering the achievement of statistical significance (p < 0.05) nearly impossible.
Part 4: Results
The meta-analysis of 11 RCTs (535 patients) yielded a shocking “negative” result across all measured fronts, entirely contradicting theoretical expectations.
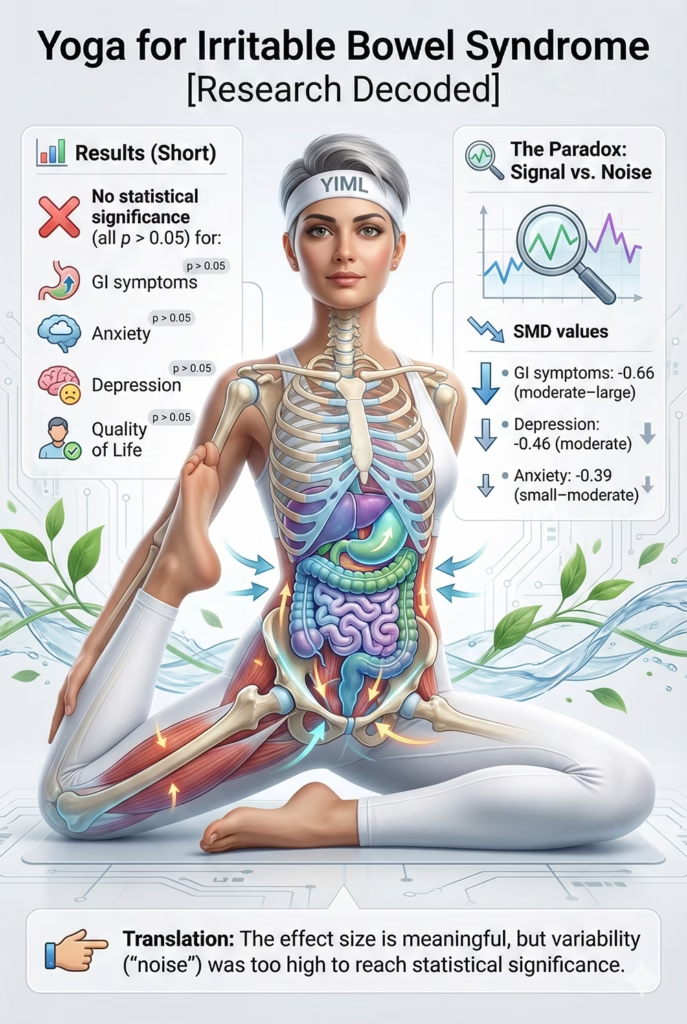
The pooled data showed NO statistically significant difference between Yoga and control groups regarding:
- Reduction of GI Symptom Severity: (SMD -0.66; 95% CI: -1.51 to 0.18; P = 0.12)
- Reduction of Anxiety: (SMD -0.39; 95% CI: -0.85 to 0.06; P = 0.09)
- Reduction of Depression: (SMD -0.46; 95% CI: -1.15 to 0.22; P = 0.19)
- Improvement in QoL: (SMD 0.53; 95% CI: -0.38 to 1.44; P = 0.25)
Decoding the Paradox: “Signal” vs. “Noise” This “negative” conclusion (all p-values > 0.05) harbors a crucial scientific paradox. A superficial reading suggests “Yoga doesn’t work.” However, a deeper look at the numbers reveals a vastly different narrative:
The “Signal”: Look at the Standardized Mean Difference (SMD) values:
- SMD for GI Symptoms: -0.66
- SMD for Depression: -0.46
- SMD for Anxiety: -0.39 (Conventionally, an SMD of 0.2 is “small,” 0.5 is “moderate,” and 0.8 is “large.”)
Layman’s translation: These numbers are not small! An SMD of -0.66 is a moderate-to-large effect. This means that, on average, Yoga actually produced a very strong, positive “signal” of improvement. Patients practicing Yoga genuinely felt better.
The “Noise”
Why did such a strong signal fail statistically (P = 0.12)? The answer lies in the 95% Confidence Interval (CI). Look at the CI for GI symptoms: -1.51 to 0.18.
Layman’s translation: This interval is massive. It essentially tells us: “Even though the average improvement was strong (-0.66), the individual studies were so wildly different from one another that we can’t be scientifically certain. The true effect might be a massive benefit (-1.51), or it might be zero, or even slightly harmful (+0.18).” Because this range crosses the zero line, the result is technically deemed “not statistically significant.”
The Paradox Conclusion: The issue here may not be a complete lack of signal. The pooled SMD values suggest a potentially meaningful clinical trend, despite failing to reach statistical significance. The issue is “Too Much Noise.” The original studies were too chaotic and heterogeneous, “breaking” the meta-analysis and preventing a definitive statistical conclusion.
Part 5: Discussion
This discussion will not focus on “Why Yoga failed?” (because it arguably didn’t). Instead, it focuses on “Why the Evidence failed?” The answer, as the authors concede, is “considerable methodological heterogeneity” and a “high risk of bias.” This is a textbook case of Garbage In, Garbage Out (GIGO).
Explaining the “Noise”: The GIGO Disaster
A meta-analysis is like a blender. If you put in “apples, oranges, and bananas” (high-quality, uniform studies), you get a reliable smoothie. If you put in “apples, bricks, and old shoes” (chaotic, low-quality studies), you get a ruined mess. This meta-analysis necessarily combined highly heterogeneous data sets:
- GIGO 1: Pooling Children with Adults. This is a fatal methodological flaw. The psychosocial drivers of IBS in a 10-year-old are vastly different from a 50-year-old. Pooling them creates massive statistical variance (noise).
- GIGO 2: Incompatible “Dosing.” Combining a 6-week intervention with an 8-month intervention is like pooling a study on 10mg of a drug with a study on 500mg and asking, “Does the drug work?”
- GIGO 3: High Risk of Bias (The Placebo Effect). In mind-body disorders like IBS, the placebo effect is incredibly powerful. The promising signal (SMD = -0.66) could be artificially inflated by patient expectation, instructor attention, and the lack of proper active control groups (e.g., comparing Yoga to a light stretching class rather than “usual care”). This is particularly relevant in conditions driven by autonomic dysregulation, similar to patterns observed in clinical research on Yoga and hypertension, where sympathetic dominance plays a central role.
Discussion Conclusion: Saab et al.’s meta-analysis does not prove Yoga is ineffective for IBS. It proves that the current landscape of Yoga research for IBS is a methodological mess, too low in quality to support definitive clinical guidelines. The statistical failure (p > 0.05) is a failure of research design, not necessarily a failure of the intervention.

Reconciling with the Brain-Gut Theory
This GIGO paradox is particularly tragic because IBS represents a condition where Yoga’s theoretical mechanisms appear highly relevant.
The positive signals (SMD = -0.66 for GI, -0.46 for Depression) support the Brain-Gut theory, suggesting Yoga impacts both ends of the axis.
- The reductions in Anxiety (p=0.09) and Depression (p=0.19) nearly reached statistical significance. Additional large, high-quality RCTs may meaningfully shift the statistical certainty of these findings. This implies the underlying theory is likely sound, but the execution of the clinical trials has been exceptionally poor.
Clinical Application (The Gastroenterologist’s Perspective)
- Reading the Abstract: If a doctor only reads the conclusion (“Yoga did not reduce…”), they will tell patients: “Don’t bother with Yoga; it doesn’t work.”
- Reading like a Scientist: If a doctor reads the full paper, they will advise: “The current science on Yoga and IBS is very messy, so official guidelines can’t endorse it yet. However, theoretically, Yoga (especially breathwork) is the perfect intervention to calm your Brain-Gut axis. Early signals show moderate-to-large benefits, and crucially, It is generally considered low-risk when appropriately supervised. It is a low-cost, low-risk adjunctive therapy highly worth trying.”
Practical Application (The Yoga Therapist’s Perspective)
- A Call for Standardization: This is a wake-up call for the Yoga community. We cannot continue teaching 100 different styles of Yoga and expect medical validation.
- Focus on the Core Mechanism: To manage IBS, Yoga protocols must hyper-focus on modulating the Brain-Gut Axis:
- PNS Activation (Priority #1): The majority of the class must be dedicated to Pranayama (specifically prolonged exhalations and diaphragmatic breathing) and profound relaxation (Yoga Nidra) to stimulate vagal tone.
- Gentle Asana: Postures should prioritize gentle abdominal massage (e.g., Pawanmuktasana / Wind-Relieving Pose, mild twists) rather than intense, heat-building Vinyasa flows, which can inadvertently spike sympathetic arousal and exacerbate IBS symptoms.
Part 6: Conclusion
The 2025 meta-analysis by Saab et al. is one of the most important papers in Yoga therapy—not because of the answer it provides, but because of the critical question it raises.
The study presents a clear dual paradox:
- The Surface Conclusion (Statistical Failure): When pooling 11 RCTs, Yoga failed to demonstrate statistically significant improvements (all p > 0.05) for GI symptoms, anxiety, depression, or QoL in IBS patients.
- The Underlying Reality (Methodological Failure): This statistical failure does not equate to clinical uselessness. It may reflect the classic “Garbage In, Garbage Out” (GIGO) phenomenon often observed in meta-analyses of heterogeneous trials.
The study actually uncovered a promising moderate-to-large “signal” of benefit (e.g., SMD = -0.66 for GI symptoms), but this signal was completely drowned out by statistical “noise” generated by pooling chaotic, heterogeneous data (mixing kids with adults, 6-week programs with 8-month programs) from highly biased trials.
This paper is not the “end” for Yoga and IBS. It is the end of the era of small, fragmented, low-quality Yoga RCTs. It is an urgent call to action: if we want to clinically validate a theoretically coherent mind-body intervention focused on Brain-Gut Axis modulation — similar to the autonomic frameworks discussed in our analysis of stress physiology and Yoga — we must demand large-scale, rigorous, and highly standardized clinical trials.
References
- Saab, O., Al-Obaidi, H., Algodi, M., Algodi, A., Rashid, Y., Al-Sagban, A., Albayyaa, M., Merza, N., Alzubaidy, L., & Cash, B. (2024). Yoga for Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. The American Journal of Gastroenterology. PMID: 40358469.
- Kennedy, D., et al. (2020). The Brain-Gut-Microbiota Axis in Irritable Bowel Syndrome. Current Gastroenterology Reports.
![The Biomechanical Demands of Standing Yoga Poses in Seniors [RESEARCH DECODED]](https://yogaismylife.vn/en/wp-content/uploads/2026/02/tu-the-chien-binh-cho-nguoi-cao-tuoi.webp)
![The Impact of Yoga on Pediatric Obesity [RESEARCH DECODED]](https://yogaismylife.vn/en/wp-content/uploads/2026/02/The-Impact-of-Yoga-on-Pediatric-Obesity.avif)

