Part I: Understanding the Pathology from Dual Perspectives
Chronic Obstructive Pulmonary Disease (COPD) is a severe, progressive respiratory condition characterized by irreversible airflow limitation. While primarily a lung disease, its systemic impact is devastating, leading to profound muscle wasting, chronic fatigue, anxiety, and a severely diminished quality of life.
Therapeutic Yoga, with its central focus on breath regulation (Pranayama), is a scientifically validated adjunctive therapy. By re-training the diaphragm, utilizing specific exhalation techniques to expel trapped air, strengthening accessory respiratory muscles, and down-regulating the nervous system, Yoga directly mitigates dyspnea (shortness of breath), improves exercise tolerance, and restores a sense of agency to the patient.
Overview of Chronic Obstructive Pulmonary Disease (COPD)
The Modern Medical Perspective COPD is an inflammatory pulmonary response to noxious particles or gases (predominantly cigarette smoke) that results in persistent, irreversible airflow obstruction.
The Core Biomechanical Issue: “Air Trapping” (Hyperinflation) In COPD, the airways narrow, and the alveolar sacs lose their elastic recoil. Consequently, air enters the lungs relatively easily but becomes “trapped” during exhalation. This chronic hyperinflation flattens the diaphragm (the primary muscle of respiration), rendering it mechanically disadvantaged and inefficient. To compensate, the body is forced to recruit accessory respiratory muscles in the neck, shoulders, and chest simply to breathe at rest. This drastically increases the metabolic work of breathing, leading to severe chronic fatigue and musculoskeletal rigidity.
Primary Phenotypes: COPD is typically an overlap of two distinct pathophysiological states:
- Chronic Bronchitis: Chronic inflammation and hypersecretion of mucus in the bronchial tubes, causing a persistent, productive cough.
- Emphysema: The irreversible destruction of the alveoli (air sacs), which severely reduces the surface area for gas exchange and destroys the lungs’ natural elasticity.
Clinical Signs and Symptoms
- Dyspnea (Shortness of breath): The hallmark symptom. Initially exertional, it progresses to occur at rest, often described as “air hunger” or chest heaviness.
- Chronic Productive Cough: Persistent coughing with significant sputum (mucus) production, especially in the morning.
- Wheezing: A whistling sound caused by air forcing its way through narrowed, inflamed airways.
- Profound Fatigue: Resulting from chronic hypoxia (low oxygen) and the massive caloric expenditure required just to breathe.
- Cyanosis: Bluish discoloration of the lips or nail beds, indicating severe systemic hypoxemia.
- Cervicothoracic Rigidity: Chronic tightness in the neck and shoulders due to the constant over-recruitment of accessory breathing muscles (scalenes, SCM, upper trapezius).
The chronic over-recruitment of accessory respiratory muscles parallels the biomechanical patterns detailed in Decoding Chronic Neck and Shoulder Pain Through Medical & Yogic Lenses: A Comprehensive Therapeutic Roadmap, reinforcing the need for targeted cervical release work.
🚨 RED FLAGS (Seek Immediate Emergency Care):
- Sudden, severe exacerbation of dyspnea unresponsive to rescue inhalers (bronchodilators).
- Profound confusion, severe lethargy, or altered mental status.
- Acute, visible cyanosis (blue lips/fingers).
- High fever or a sudden change in sputum color (yellow/green) accompanying worsening breathlessness.
The Yogic and Ayurvedic Perspective
Ayurveda views COPD (Pranavaha Srotodushti—disorder of the Prana-carrying channels) as a profound systemic imbalance primarily driven by aggravated Kapha (causing obstruction) and Vata (causing dryness and spasms).
1. Dosha Imbalance
- Aggravated Kapha (Chronic Bronchitis Phenotype): The cold, wet, heavy qualities of Kapha produce excessive, sticky mucus (Ama). This physical stagnation clogs the airways, causing chronic coughing, a feeling of heaviness in the chest, and obstructed breathing.
- Aggravated Vata (Emphysema Phenotype): The dry, light, rough qualities of Vata induce tissue desiccation and atrophy (Dhatu Kshaya) of the alveoli, destroying their elasticity. High Vata also triggers bronchial spasms and the acute psychological anxiety/fear associated with breathlessness.
2. Disruption of Prana Vayus (Energy Currents)
- Blocked Prana Vayu & Udana Vayu: Prana Vayu (inward-moving energy in the chest) is mechanically obstructed, preventing the absorption of vital life force. Udana Vayu (upward-moving energy in the throat) is choked by Kapha mucus and Vata spasms, resulting in chronic coughing and a suffocating reversal of energy flow.
- Weakened Apana Vayu: The panic of breathlessness chronically weakens Apana Vayu (the grounding, downward-moving energy). This prevents the diaphragm from descending properly, trapping the patient in a cycle of shallow, anxious upper-chest breathing.

3. Chakra Stagnation
- Anahata Chakra (Heart): The physical congestion (mucus/hyperinflation) and emotional stagnation (grief, fear of suffocation, isolation) severely block energy flow here, manifesting as chest heaviness and profound fatigue.
- Vishuddha Chakra (Throat): Chronically irritated by coughing, mucus production, and the rigid contraction of accessory neck muscles, creating severe energetic stagnation in the upper respiratory tract.
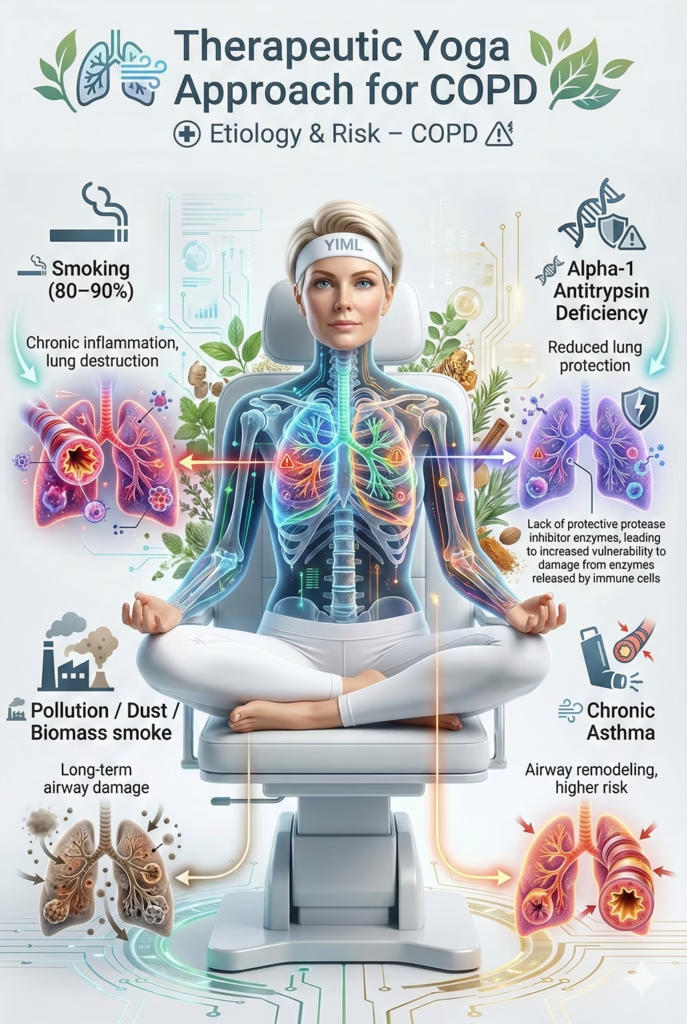
Etiology and Risk Factors
The Modern Medical Perspective
- Primary Environmental Driver: Cigarette smoking accounts for 80-90% of cases, causing irreversible inflammatory destruction of lung architecture.
- Occupational/Environmental Exposure: Long-term exposure to severe air pollution, biomass cooking smoke (especially in poorly ventilated areas), and industrial dust/chemicals.
- Genetic Factors: Alpha-1 antitrypsin deficiency (a rare genetic lack of a lung-protecting protein).
- Chronic Asthma: Can structurally remodel the airways over time, increasing COPD risk.
The Ayurvedic Perspective Beyond noxious inhalants, a lifestyle that aggravates Kapha (sedentary behavior, excessive consumption of cold/heavy/sweet foods) and Vata (erratic schedules, chronic stress, consumption of dry/cold foods) sets the systemic foundation for the disease to take root and progress rapidly when exposed to environmental toxins.
Part II: The Therapeutic Yoga Approach for COPD
Therapeutic Goals The therapeutic yoga approach for COPD is a comprehensive strategy targeting respiratory mechanics, dyspnea management, breaking the dyspnea-anxiety cycle, and improving overall Quality of Life (QoL). These objectives are robustly supported by clinical evidence.
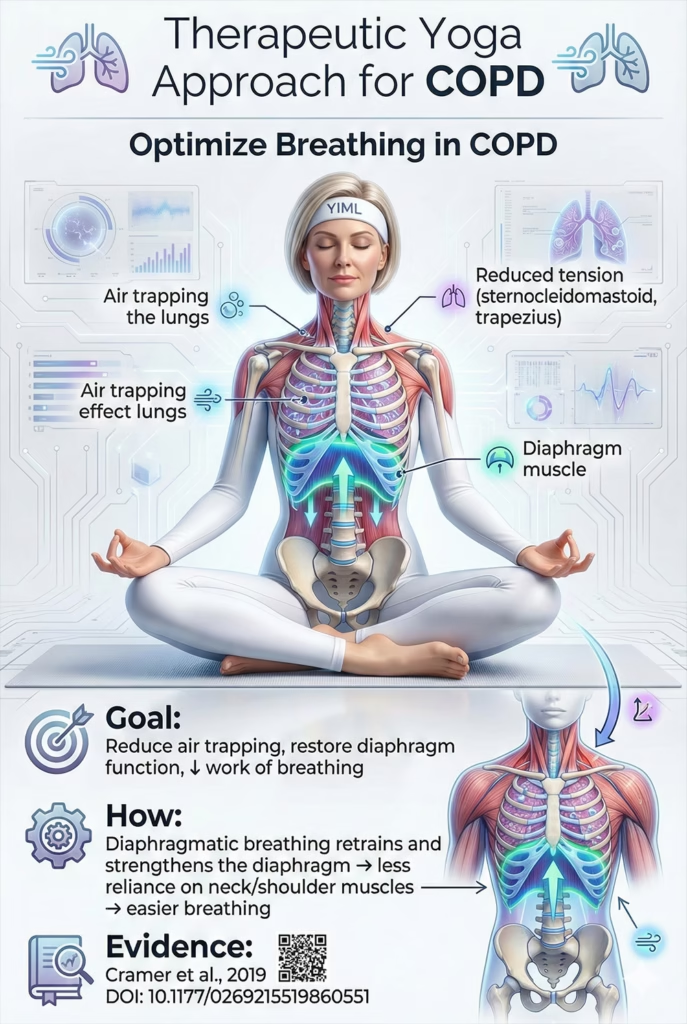
1. Optimize Breathing Mechanics & Strengthen the Diaphragm
- The Goal:The fundamental mechanical objective. In COPD, “air trapping” hyperinflates the lungs, pushing the diaphragm (the primary respiratory muscle) downward into a flattened, mechanically disadvantaged position. This forces the body to over-rely on accessory muscles (neck and shoulders), substantially increasing metabolic demand and the Work of Breathing (WOB).
- Mechanism: Therapeutic Yoga focuses on neuromuscular re-education of the diaphragm via structured diaphragmatic breathing. By consciously expanding the abdomen on inhalation, the patient actively recruits and strengthens the diaphragm, improving its excursion and mechanical efficiency. Evidence from a systematic review and meta-analysis indicates that yoga interventions improve pulmonary function and reduce symptom burden in individuals with COPD, supporting its role in optimizing breathing mechanics and reducing dyspnea (Cramer et al., 2019 DOI: 10.1177/0269215519860551).
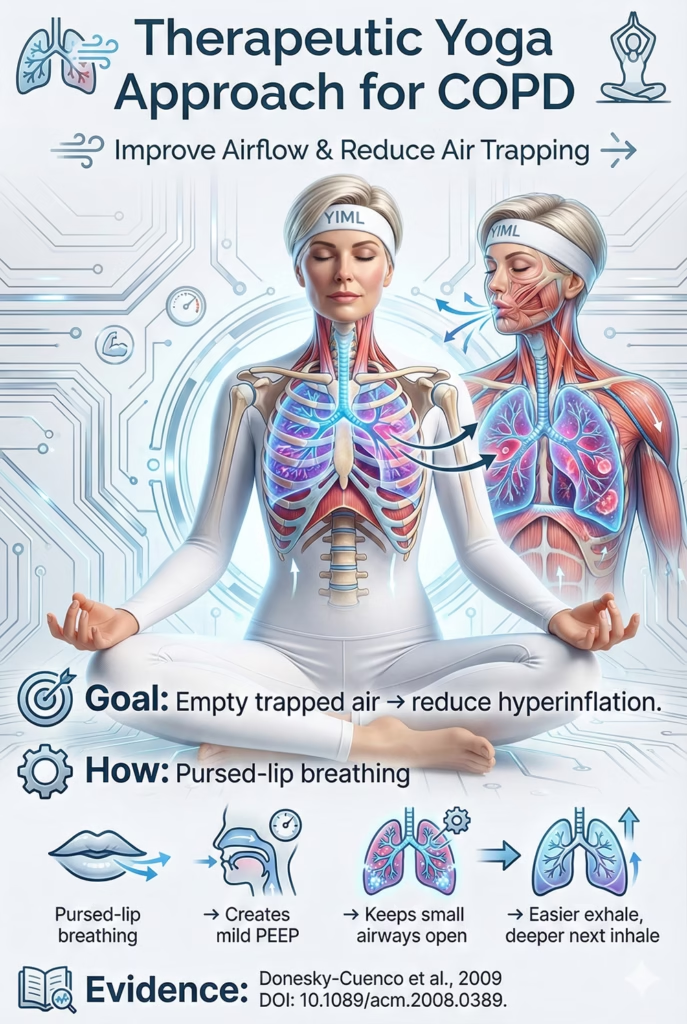
2. Improve Airflow & Reduce Air Trapping
- The Goal: To facilitate effective exhalation, expelling trapped air and reducing pulmonary hyperinflation.
- Mechanism: Yoga heavily utilizes Pursed-Lip Breathing, which is also the gold standard in pulmonary rehabilitation. Exhaling against pursed lips creates mild Positive End-Expiratory Pressure (PEEP) within the airways. This internal pressure acts as a “pneumatic splint,” preventing the premature collapse of small, floppy airways. This allows trapped air to escape, helping the diaphragm return to a more optimal resting position and making the subsequent inhalation deeper and less effortful (Donesky-Cuenco et al., 2009 DOI: 10.1089/acm.2008.0389).
3. Break the Dyspnea-Anxiety Cycle
- The Goal: Dyspnea (air hunger) is a terrifying sensation that instantly triggers a sympathetic panic response. Panic induces bronchospasm and rapid, shallow breathing (tachypnea), which exponentially worsens air trapping—creating a vicious cycle.
- Mechanism: Yoga directly interrupts this loop. Techniques utilizing prolonged exhalations (Pursed-Lip Breathing) and deep relaxation (Savasana) forcefully stimulate the vagus nerve, inducing parasympathetic dominance (“rest and digest”). This physiological shift lowers the heart rate, extinguishes acute anxiety, and promotes mild bronchodilation. Most importantly, it arms the patient with a proactive coping mechanism to remain calm during an exacerbation.
This dyspnea–panic loop reflects the broader mechanisms of sympathetic overactivation explored in our roadmap on stress and nervous system rebalancing through yoga therapy, where breath regulation serves as the primary autonomic gateway.

4. Release Accessory Muscle Tension & Improve Posture
- The Goal: Chronic over-recruitment of accessory respiratory muscles leads to severe rigidity in the neck, shoulders, and chest. The resulting kyphotic (hunched) posture structurally compresses the ribcage, further restricting lung expansion.
- Mechanism: Yoga employs highly targeted, gentle mobilization (especially Chair Yoga) to release myofascial tension in the scalenes, sternocleidomastoid (SCM), upper trapezius, and pectorals. Passive chest-opening postures and mild upper-back strengthening counteract kyphosis. Correcting this posture mechanically expands the thoracic cavity, giving the lungs and diaphragm more physical space to operate (Li et al., 2018 DOI: 10.1016/j.ctcp.2017.11.006).

5. Improve Exercise Tolerance & Quality of Life
- The Goal: Patients often fall into a debilitating “deconditioning spiral”: Dyspnea ➔ Fear of movement ➔ Sedentary lifestyle ➔ Muscle atrophy ➔ Worse dyspnea upon minimal exertion.
- Mechanism: Yoga (particularly Chair Yoga) provides an exceptionally safe, low-impact method for systemic reconditioning. Strengthening the peripheral musculature (arms and legs) improves their oxygen extraction efficiency. Consequently, stronger muscles require less oxygen to perform daily tasks, thereby reducing the overall ventilatory demand on the compromised lungs.

Golden Rules & Absolute Contraindications for COPD
CRITICAL WARNING: COPD is a severe, life-threatening medical condition. This therapeutic yoga guide is strictly an adjunctive therapy and must never replace protocols prescribed by your pulmonologist or respiratory therapist. Always consult your physician before initiating any exercise regimen, and always keep your rescue inhaler (short-acting bronchodilator) within reach during practice.
The Golden Rules of Practice
1. Dyspnea is the Absolute Stop Signal
- The Rule: You must learn to differentiate between “muscular fatigue” and “dyspnea” (air hunger, chest tightness, or respiratory distress). If you experience worsening breathlessness, dizziness, or palpitations, STOP IMMEDIATELY.
- Action: Sit down, relax your shoulders, and initiate Pursed-Lip Breathing until your respiratory rate normalizes. Pushing through dyspnea in COPD does not build endurance; it induces severe hypoxemia, triggers panic-induced bronchospasm, and can precipitate an acute exacerbation.
2. The Exhale is the Key (Pursed-Lip Breathing)
- The Rule: Your primary focus must always be extending the exhalation to be longer than the inhalation.
- Mechanism: Actively utilize Pursed-Lip Breathing (inhale through the nose, exhale slowly through pursed lips as if blowing out a candle) throughout the entire practice, especially during any exertion. This creates mild Positive End-Expiratory Pressure (PEEP), splinting the airways open to expel trapped air, thereby reducing hyperinflation and making room for the next inhalation.
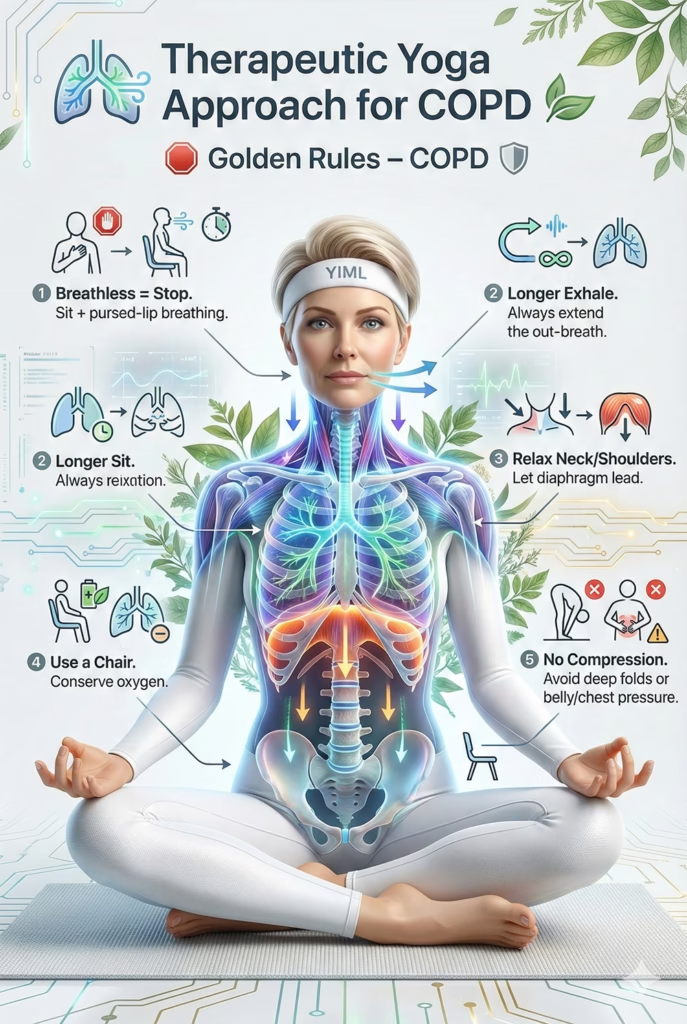
3. Release the Cervicothoracic Musculature
- The Rule: Consciously un-shrug and relax the neck, shoulders, and upper chest.
- Mechanism: In COPD, the flattened diaphragm forces the accessory respiratory muscles (scalenes, SCM, upper trapezius) to overwork. Yoga must focus on releasing this myofascial rigidity. Relieving this tension reduces the wasted work of breathing and mechanically allows the diaphragm to re-engage.
4. Props are Mandatory (Especially the Chair)
- The Rule: The chair is your primary therapeutic tool. Prioritize seated postures or standing postures using the chair for balance.
- Mechanism: Unsupported standing postures demand significant metabolic energy for balance and postural stabilization, which drives up oxygen consumption. Seated practices offload this energy expenditure, allowing you to allocate your limited oxygen reserves entirely to conscious breathing and gentle peripheral conditioning.
5. Avoid Abdominal & Thoracic Compression
- The Rule: Avoid deep forward folds or prone (face-down) positions that compress the abdomen or restrict the ribcage.
- Mechanism: The diaphragm requires physical space to descend during inhalation. Any external pressure on the abdomen (e.g., compressing the thighs into the belly) or the anterior chest wall mechanically impedes diaphragmatic excursion, triggering immediate and severe dyspnea.
Absolute Contraindications (What to Avoid)
To ensure absolute respiratory safety, individuals with COPD must STRICTLY AVOID the following actions and postures.
1. Severe Inversions (Head Below Heart)
- Avoid: Downward-Facing Dog (Adho Mukha Svanasana), Deep Forward Folds (Uttanasana), Shoulderstand, Plow.
- Scientific Rationale: In these gravity-inverted positions, the weight of the abdominal viscera (organs) presses heavily against the diaphragm from below. This severely restricts the diaphragm’s ability to contract downward, drastically reducing inspiratory capacity and inducing acute, severe dyspnea in an already compromised respiratory system.
2. Prone Postures (Belly/Chest on the Floor)
- Avoid: Locust (Salabhasana), Bow (Dhanurasana), or unsupported Cobra.
- Scientific Rationale: Direct compression of the anterior chest wall and abdomen physically restricts ribcage expansion and diaphragmatic descent, exponentially increasing the work of breathing.
- Safe Alternative: Perform all chest-opening extensions while seated in a chair or in a highly propped, supine (face-up) position.
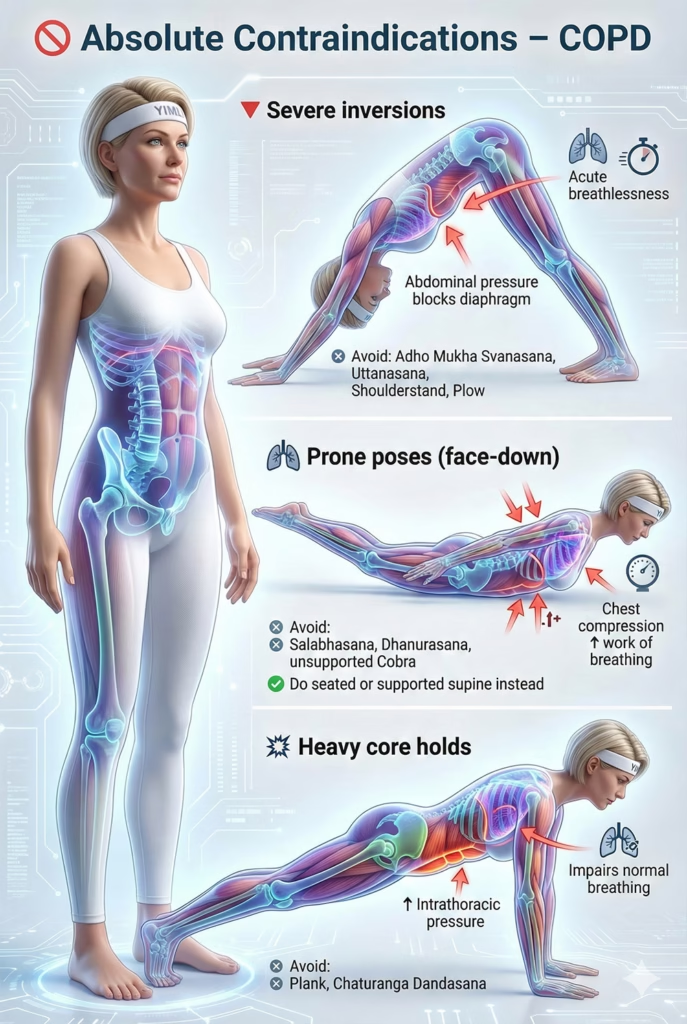
3. Intense Isometric Holds & Heavy Core Bracing
- Avoid: Plank, Chaturanga Dandasana, and arm balances.
- Scientific Rationale: These postures inherently require the Valsalva maneuver (bearing down) or intense core bracing. This spikes intrathoracic pressure and directly impedes normal respiration.
4. Breath Retention (Kumbhaka)
- Avoid: Holding the breath after inhalation or exhalation.
- Scientific Rationale: This is an absolute contraindication. Breath retention increases intrathoracic pressure, places immense strain on the cardiovascular system (which is often already compromised by cor pulmonale in COPD), and can trigger severe bronchospasm. It also rapidly exacerbates panic associated with air hunger.
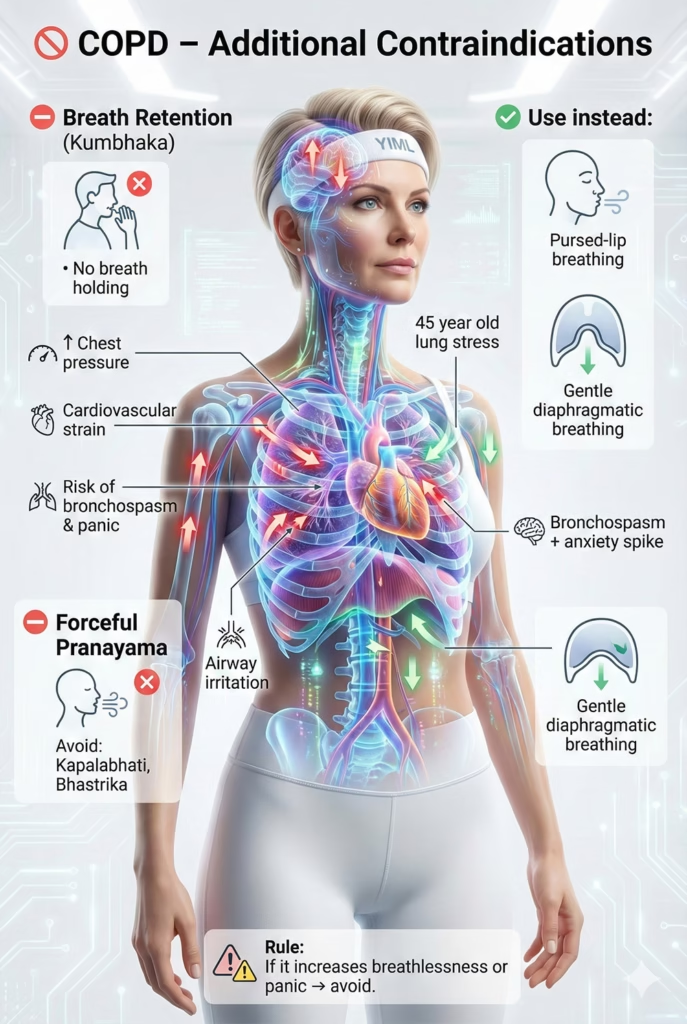
5. Forceful, Hyperventilatory Pranayama
- Avoid: Kapalabhati (Breath of Fire), Bhastrika (Bellows Breath).
- Scientific Rationale: Rapid, forceful exhalations can irritate hyper-reactive airways, inducing severe bronchospasm and triggering an acute dyspneic attack. Furthermore, hyperventilation drives sympathetic nervous system arousal (anxiety/panic).
- Safe Alternative: Strictly utilize Pursed-Lip Breathing and gentle Diaphragmatic Breathing.
Summary: Any posture or breathing technique that increases dyspnea, mechanically compresses the chest/abdomen, requires breath holding, or induces panic must be categorically avoided. Safety, prolonged exhalations, and anatomical support are the non-negotiable pillars of this practice.
Part III: Detailed Therapeutic Yoga Toolkit for COPD
A. Asana (Postures)
General Reminder: The objective is respiratory efficiency and tension release, not exertion. Move excruciatingly slow, synchronize every movement with Pursed-Lip Breathing, and STOP IMMEDIATELY if dyspnea increases. The chair is your most vital piece of equipment.
Module 1: Mobilization & Tension Release (Seated) Target: To mobilize the thoracic spine, release chronic tension in accessory respiratory muscles, and establish a controlled respiratory rate.
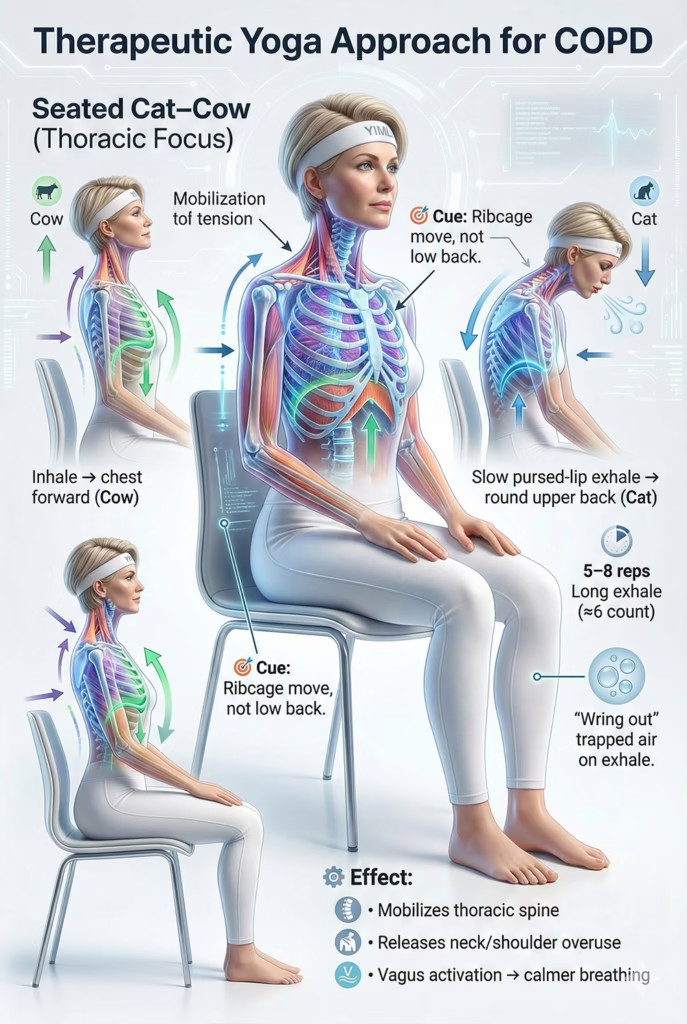
1. Seated Cat-Cow (Thoracic Mobilization)
- Technique: Sit firmly on a chair. Inhale through the nose, gently drawing the sternum forward (Cow). Exhale very slowly through pursed lips, rounding only the upper back and dropping the chin slightly (Cat). Repeat 5-8 times.
- Therapeutic Mechanism: Mobilizes the rigid thoracic spine and stretches overworked accessory muscles without the metabolic cost of quadruped positions.
- Safety Protocol: * RED FLAG: Stop immediately if dizziness or panic occurs.
- Exhalation must be via pursed lips.
- Keep movements small; do not fold deeply forward to avoid compressing the diaphragm.
For a detailed EMG and spinal loading analysis of this movement pattern, see Marjaryasana–Bitilasana (Cat–Cow Pose): Benefits, Biomechanics, and Safe Step-by-Step Guide for Beginners & Therapists.
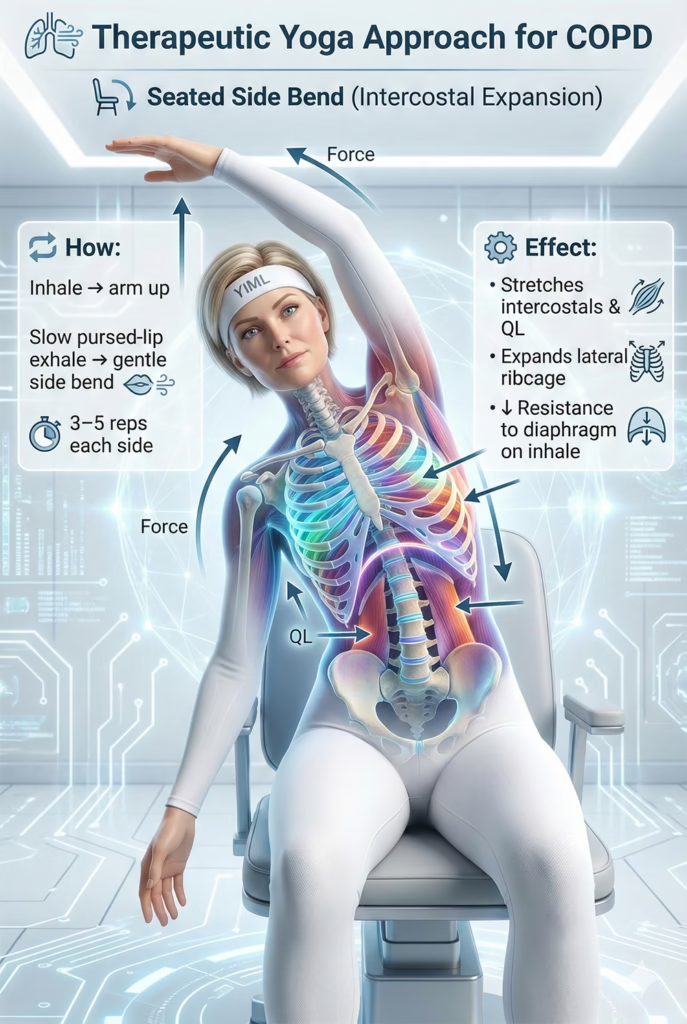
2. Seated Side Bend (Intercostal Expansion)
- Technique: Anchor the right hand to the chair. Inhale, reach the left arm up. Exhale slowly through pursed lips, bending gently to the right. Inhale back to center. Repeat 3-5 times per side.
- Therapeutic Mechanism: Stretches the intercostal muscles, physically expanding the lateral ribcage to reduce mechanical resistance during inhalation.
- Safety Protocol: * Pursed-lip exhalation is mandatory during the lateral bend (the exertion phase).
- Keep the head strictly neutral (eyes forward); do not flex or extend the cervical spine.
- Do not lean forward off the coronal plane.
Module 2: Safe Strengthening (Seated) Target: To safely condition peripheral muscles (arms and legs) to improve oxygen extraction efficiency without overtaxing the compromised pulmonary system.
3. Seated Leg Extension (Quadriceps Conditioning)
- Technique: Inhale through the nose. Exhale slowly through pursed lips while extending the right leg forward. Inhale to lower. Repeat 5-8 times per leg.
- Therapeutic Mechanism: Combats peripheral muscle wasting. Stronger legs extract oxygen more efficiently, reducing the overall ventilatory demand on the lungs.
- Safety Protocol:
- Synchronization is critical: Initiate the pursed-lip exhale before extending the leg.
- Do not lock the knee joint.
- Keep the back supported against the chair to keep the chest open.

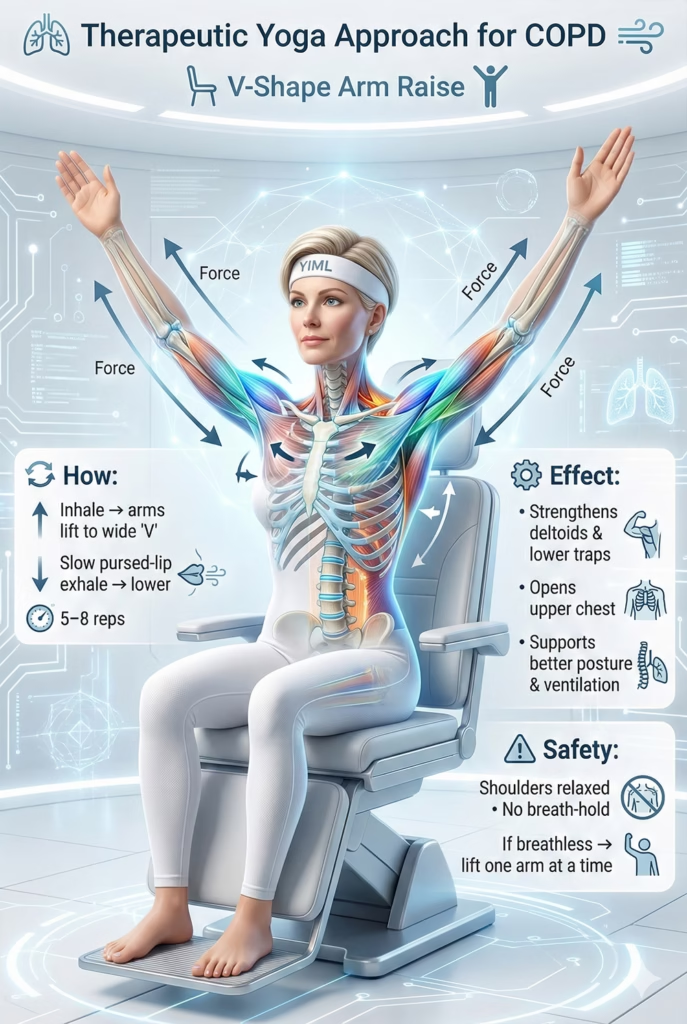
4. Seated V-Shape Arm Raise (Thoracic Expansion)
- Technique: Inhale, float both arms forward and up into a wide “V”. Exhale slowly through pursed lips, lowering the arms. Repeat 5-8 times.
- Therapeutic Mechanism: Strengthens shoulder elevators to correct kyphosis and mechanically expands the upper ribcage.
- Safety Protocol: * Keep shoulders relaxed away from the ears (do not shrug).
- Never hold the breath. * If lifting both arms triggers dyspnea, modify by lifting only one arm at a time.
Module 3: Targeted Myofascial Release (Seated) Target: To passively stretch the specific accessory muscles that become hypertonic (spastic) from the constant work of breathing.
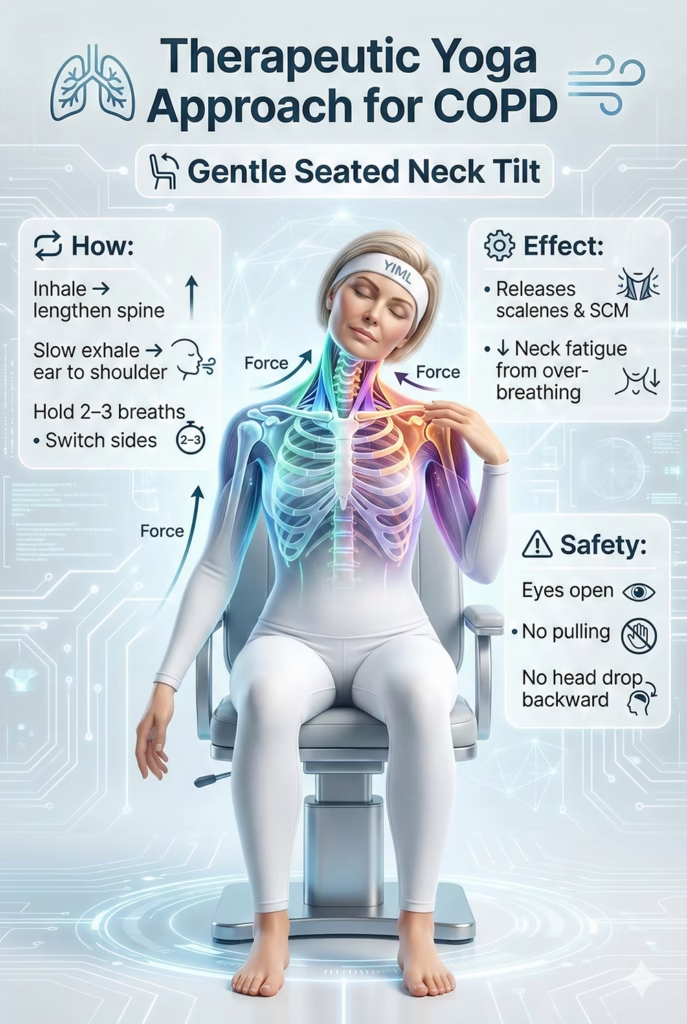
5. Gentle Seated Neck Tilt (Scalene/SCM Release)
- Technique: Sit upright, arms heavy at the sides. Inhale, lengthen the crown upward. Exhale through pursed lips, gently dropping the right ear toward the right shoulder. Hold for 2-3 breath cycles. Switch sides.
- Therapeutic Mechanism:
- Biomechanical: Directly releases the scalenes and sternocleidomastoid (SCM)—the primary accessory muscles that heave the ribcage upward during COPD-induced respiratory distress. Releasing them drastically reduces cervical fatigue.
- Safety Protocol: Keep eyes open (a fixed Drishti) to prevent vertigo. Never use the hand to pull the head; let gravity do the work. Never tilt the head backward into extension.
6. Seated Chest Opener (Pectoral Release)
- Technique: Reach arms behind the chair. Inhale, roll shoulders back, squeezing scapulae together. Exhale slowly through pursed lips. Hold 3-5 breaths.
- Therapeutic Mechanism: Counteracts hunched posture, un-restricting the anterior chest wall to give the diaphragm room to descend.
- Safety Protocol: * Do not drop the head backward; keep the chin parallel to the floor.
- Engage the core lightly to prevent hyper-extending the lower back.

Module 4: Restorative Poses Target: To induce profound parasympathetic dominance, utilizing props to passively expand the ribcage, minimizing the work of breathing, and facilitating systemic rest.
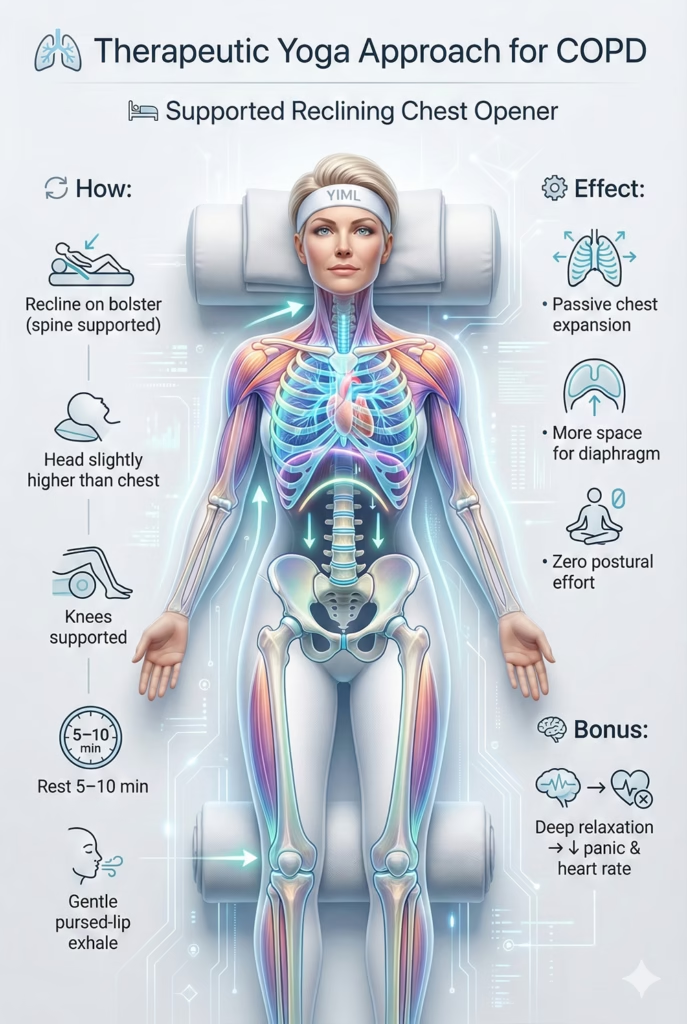
7. Supported Reclining Chest Opener
- Technique: Place a bolster longitudinally on the mat. Sit in front and recline. Ensure the head is elevated slightly higher than the chest. Place a rolled blanket under the knees. Rest for 5-10 minutes.
- Therapeutic Mechanism: Passively expands thoracic volume without muscular effort. Sends massive safety signals to the brain, extinguishing sympathetic panic.
- Safety Protocol:
- Head Elevation is Mandatory: The head must be supported to keep the airway open.
- Maintain gentle pursed-lip exhalations even while resting.
- Keep warm with a blanket (cold triggers bronchospasm).
- Exit slowly: Bend knees, roll gently to one side, and use arms to push up. Do not sit straight up.
B. Pranayama (Breathwork)
General Reminder: For COPD, breathing exercises are the paramount therapeutic tool. The goals are strictly to improve exhalatory efficiency (clearing trapped air), recondition the diaphragm, and sedate the nervous system to break the dyspnea-anxiety loop. Breath retention (Kumbhaka) is absolutely prohibited.
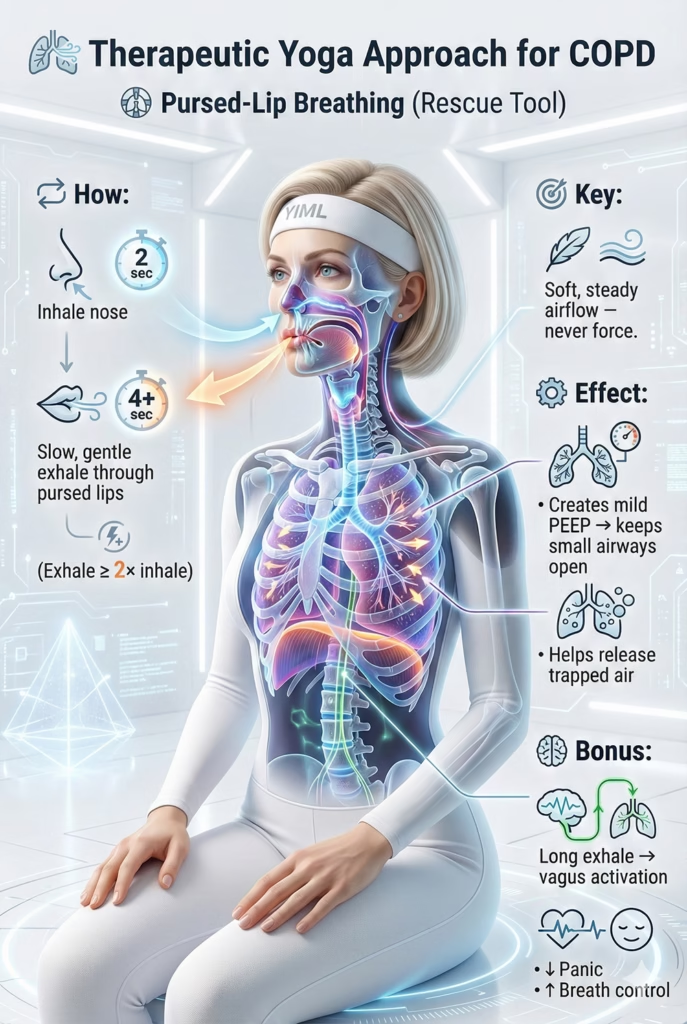
1. Pursed-Lip Breathing (The Rescue Tool)
- Technique: Sit comfortably with back support. Relax the neck and shoulders. Inhale slowly through the nose for 2 seconds. Purse the lips (as if preparing to blow out a candle). Exhale very slowly and evenly through the pursed lips, making the exhale at least twice as long as the inhale (4+ seconds).
- Instructor’s Cue: “This is your ultimate rescue tool. The secret is the gentleness of the exhale. Do not blow forcefully. Imagine blowing a feather just enough to keep it afloat, not blowing out a candle. This slow, steady stream of air creates internal back-pressure, splinting your airways open so trapped air can finally escape. This is how you reclaim control of your breath.”
- Therapeutic Mechanism:
- Biomechanical: The core pathology of COPD is the premature collapse of small airways during exhalation, causing air trapping. Pursed-Lip Breathing generates mild Positive End-Expiratory Pressure (PEEP) inside the bronchial tree. This pressure acts as a pneumatic stent, keeping the floppy airways open and facilitating the complete expulsion of stale air.
- Neurological: Dyspnea instantly triggers the sympathetic “fight-or-flight” response. Deliberately slowing the respiratory rate and extending the exhale forcefully engages the vagus nerve, driving parasympathetic dominance to extinguish acute panic.
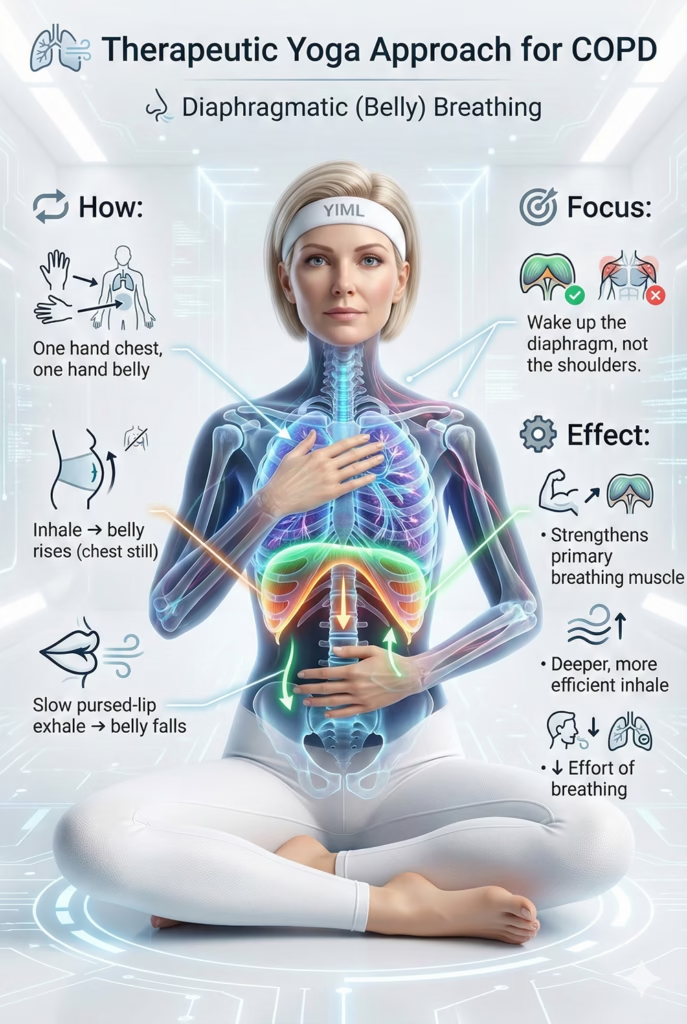
2. Diaphragmatic Breathing (Belly Breathing)
- Technique: Lie supine with knees bent, or sit well-supported. Place one hand on the upper chest, the other on the abdomen (just below the ribs). Inhale slowly through the nose, focusing entirely on making the abdomen rise (pushing the lower hand up) while keeping the chest hand completely still. Exhale slowly via pursed lips, letting the abdomen fall.
- Instructor’s Cue: “In COPD, the diaphragm goes to sleep, and the neck and shoulders take over. We are waking the diaphragm back up. At first, this will feel incredibly unnatural because your body is used to heave-breathing with the chest. Be patient. Let the hand on your chest be a strict reminder: no movement here. It takes weeks to retrain this muscle, but it is the greatest investment in your respiratory health.”
- Therapeutic Mechanism:
- Biomechanical: Re-conditions the primary respiratory muscle. A stronger diaphragm pulls further down into the abdominal cavity, generating greater negative intrathoracic pressure to draw air deeply into the lung bases with significantly less metabolic effort than accessory muscle breathing.
C. Meditation & Deep Relaxation
General Reminder: These are potent tools to reprogram the brain’s panic response to breathlessness. Always practice in fully supported, safe positions (never lying flat on the back without elevation).
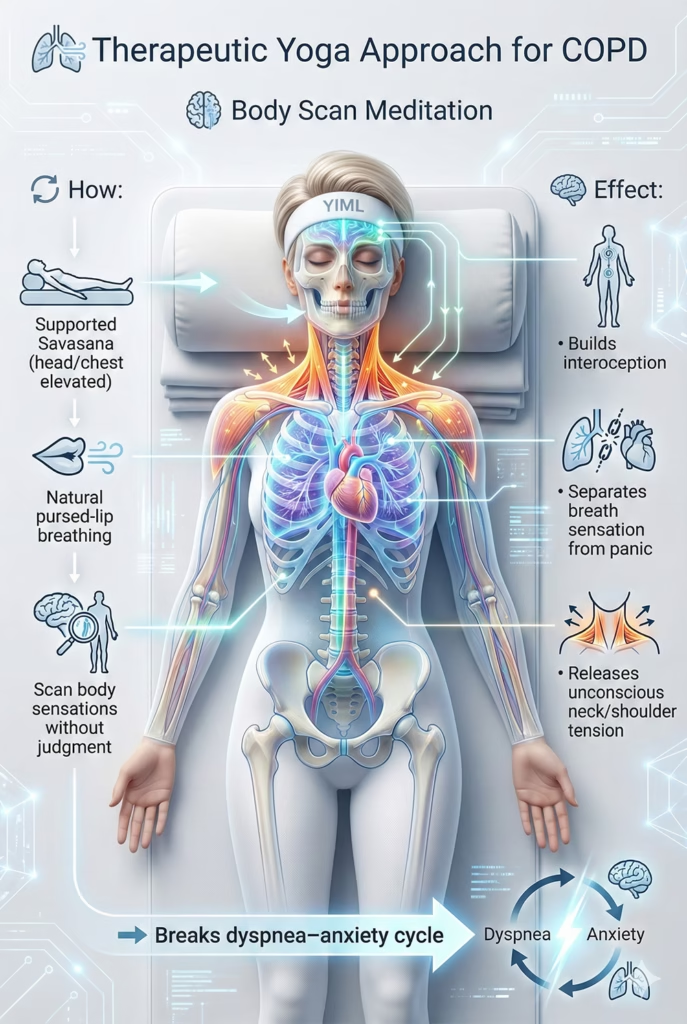
1. Body Scan Meditation
- Technique: Rest in Supported Savasana (head and chest elevated higher than the abdomen on a wedge or bolster). Close eyes and maintain natural pursed-lip breathing. Systematically move your awareness through the body, observing sensations without judgment.
- Therapeutic Mechanism:
- Neurological: Trains interoception (internal body awareness). It teaches the brain to observe the physical sensation of dyspnea objectively, decoupling it from the emotional terror of suffocation. This breaks the vicious “dyspnea-anxiety” cycle. It also helps patients identify and consciously release unconscious accessory muscle guarding.
2. Metta (Loving-Kindness) Meditation
- Technique: Sit supported or recline. Focus on the heart center. Silently repeat phrases of goodwill, directing them specifically to the respiratory system (e.g., “May my lungs heal. May I breathe with ease. May I be at peace.”).
- Therapeutic Mechanism:
- Psychological: Chronic respiratory distress breeds anger, fear, and a sense of betrayal toward one’s own body. Metta meditation cultivates radical self-compassion, shifting the internal environment from hostility to care, which actively lowers systemic stress hormones.

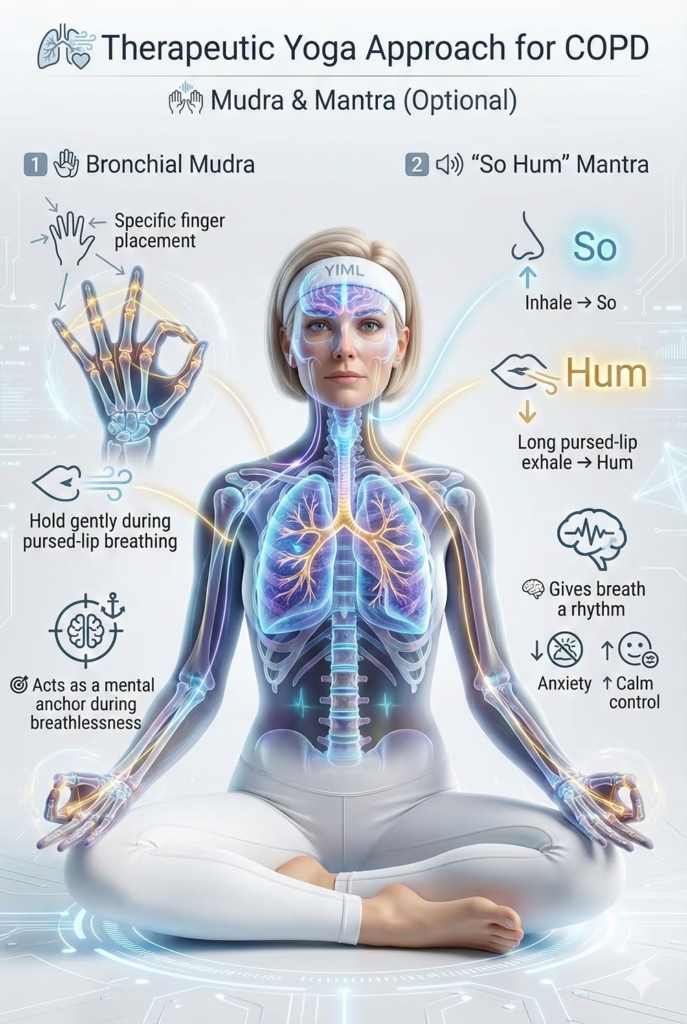
D. Mudra & Mantra (Optional Integration)
These subtle practices serve as focal anchors for the mind during respiratory distress.
1. Bronchial Mudra
- Technique: Place the tip of the pinky finger at the base of the thumb. Place the ring fingertip on the middle thumb joint. Place the middle fingertip on the tip of the thumb. Extend the index finger. Rest the backs of the hands on the thighs.
- Instructor’s Cue: “Hold this specialized respiratory mudra gently. Pair it with your Pursed-Lip Breathing. It acts as a physical anchor for your mind to focus on while your breath stabilizes.”
2. “So Hum” Mantra (I Am That)
- Technique: Recline supported. Sync the mantra with the breath. On the nasal inhale, silently chant “So”. On the pursed-lip exhale, silently chant the long, vibrating sound of “Hum”.
- Instructor’s Cue: “Let this mantra become the rhythm of your breath. ‘So’ is the inhale. ‘Hum’ rides the long exhale. Let the ‘Hum’ drag out smoothly, carrying all the trapped air and anxiety out with it. When the mind has a rhythmic anchor like this, it stops panicking about the next breath.”
Part IV: Integration & Practice Protocols for COPD
WARNING: This sequence is purely suggestive and must be meticulously adapted to your daily dyspnea threshold. Always consult your pulmonologist before initiating practice. Stop immediately if breathlessness, dizziness, or panic increases. Keep your rescue bronchodilator within reach.
Suggested 20-Minute Respiratory Support Sequence
Preparation (1 min): Ensure the room is warm (cold air triggers bronchospasm). Have a sturdy chair, pillows, and blankets ready. Move excruciatingly slow; let the exhale dictate the pace.
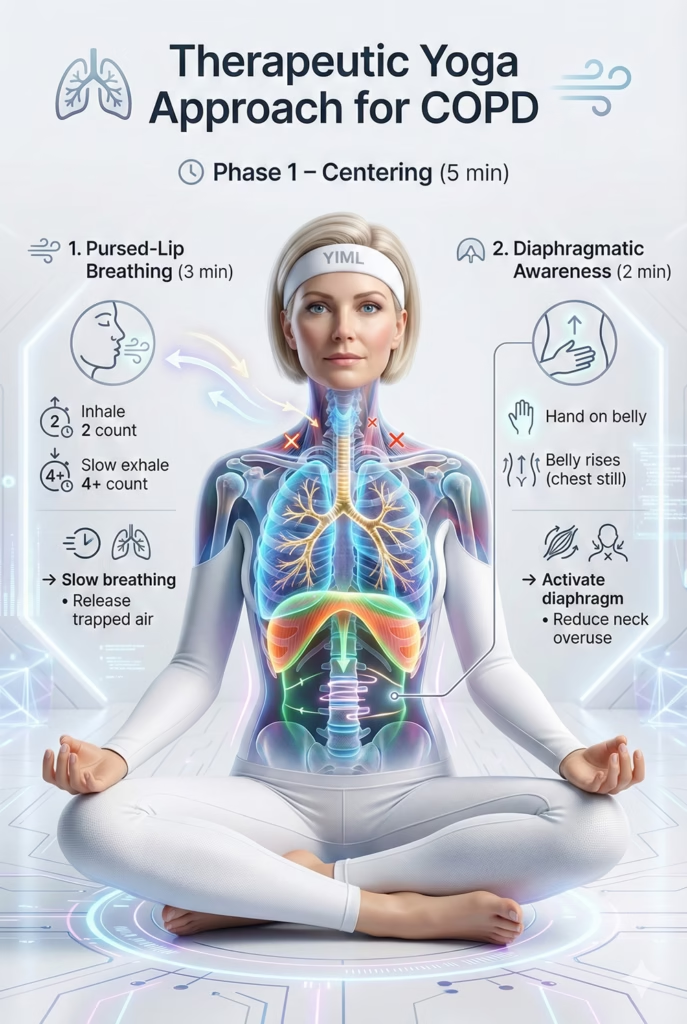
Phase 1: Centering & Establishing the Breath (5 Minutes)
1. Seated Pursed-Lip Breathing (3 mins)
- Technique: Sit supported. Relax shoulders. Inhale gently via the nose (count 1, 2). Purse lips. Exhale very slowly (count 1, 2, 3, 4+).
- Goal: Immediately establishes respiratory control, slows tachypnea (rapid breathing), and clears trapped air.
2. Diaphragmatic Awareness (2 mins)
- Technique: Place one hand on the belly. Inhale, focusing strictly on expanding the belly. Exhale via pursed lips, letting the belly fall. Keep the chest completely still.
- Goal: “Wakes up” the diaphragm and suppresses accessory muscle breathing.
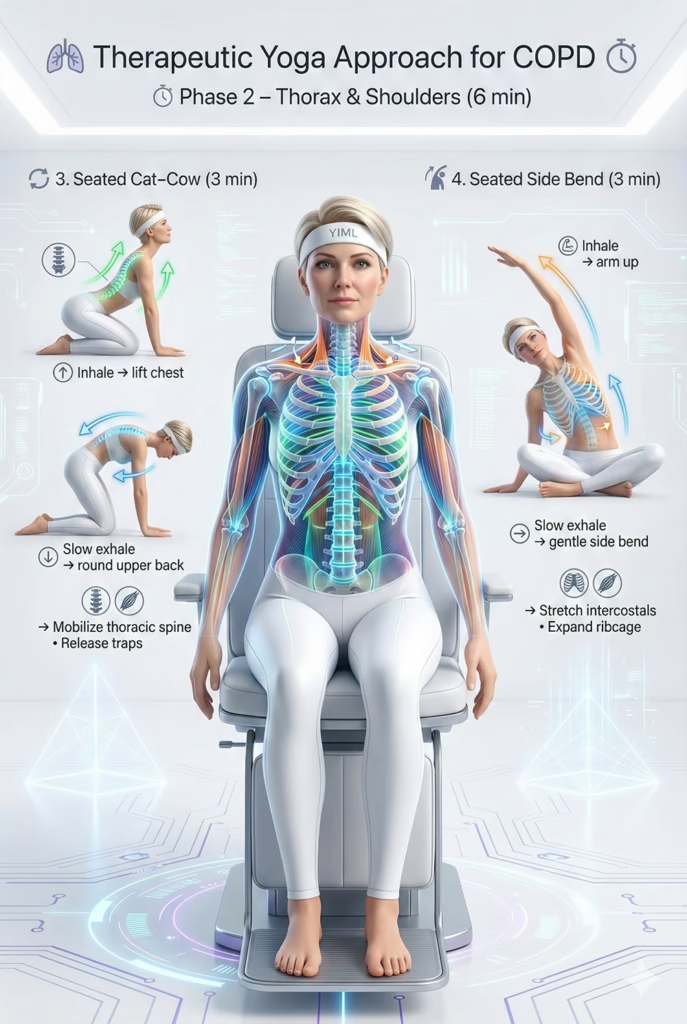
Phase 2: Mobilizing the Thorax & Shoulders (6 Minutes)
3. Seated Cat-Cow (Micro-Movements) (3 mins)
- Technique: Inhale, gently lift the sternum. Exhale (pursed lips), round the upper back slightly. Repeat 5-6 times.
- Goal: Mobilizes the thoracic spine and releases the upper trapezius.
4. Gentle Seated Side Bend (3 mins)
- Technique: Inhale, reach one arm up. Exhale (pursed lips), lean gently to the side. Repeat 3 times per side.
- Goal: Stretches the intercostals, mechanically expanding the ribcage for better ventilation.
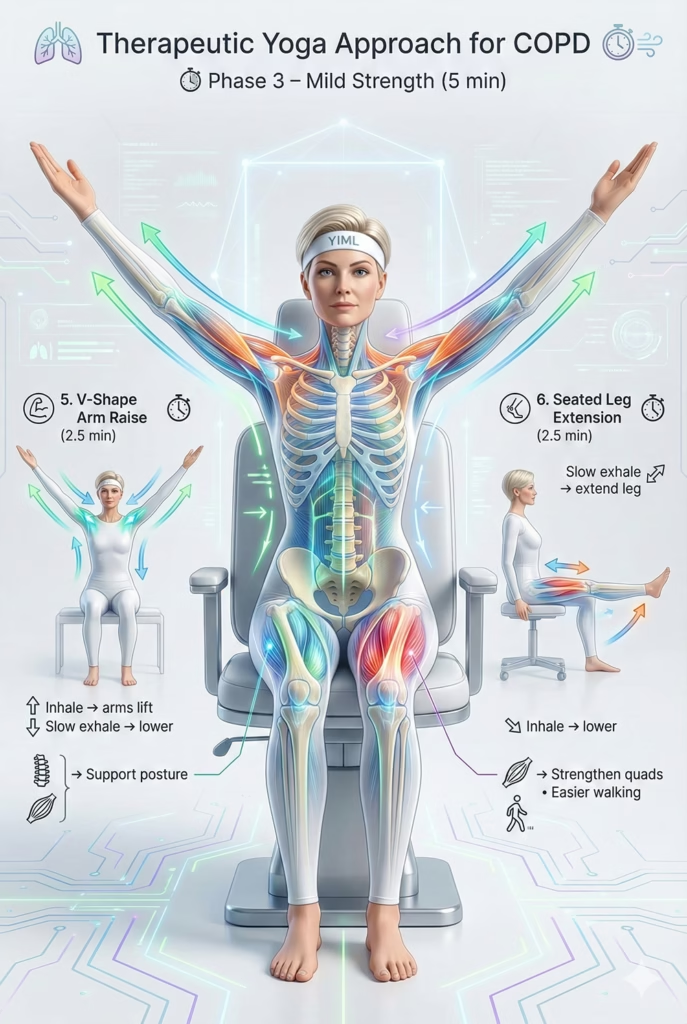
Phase 3: Mild Peripheral Strengthening (5 Minutes)
5. Seated V-Shape Arm Raise (2.5 mins)
- Technique: Inhale, float arms up into a “V”. Exhale (pursed lips), lower slowly. Repeat 5-8 times.
- Goal: Conditions shoulder elevators to improve posture without inducing dyspnea.
6. Seated Leg Extension (2.5 mins)
- Technique: Exhale (pursed lips) while extending one leg straight. Inhale to lower. Repeat 5-8 times per leg.
- Goal: Combats quadriceps atrophy, making walking less metabolically demanding.
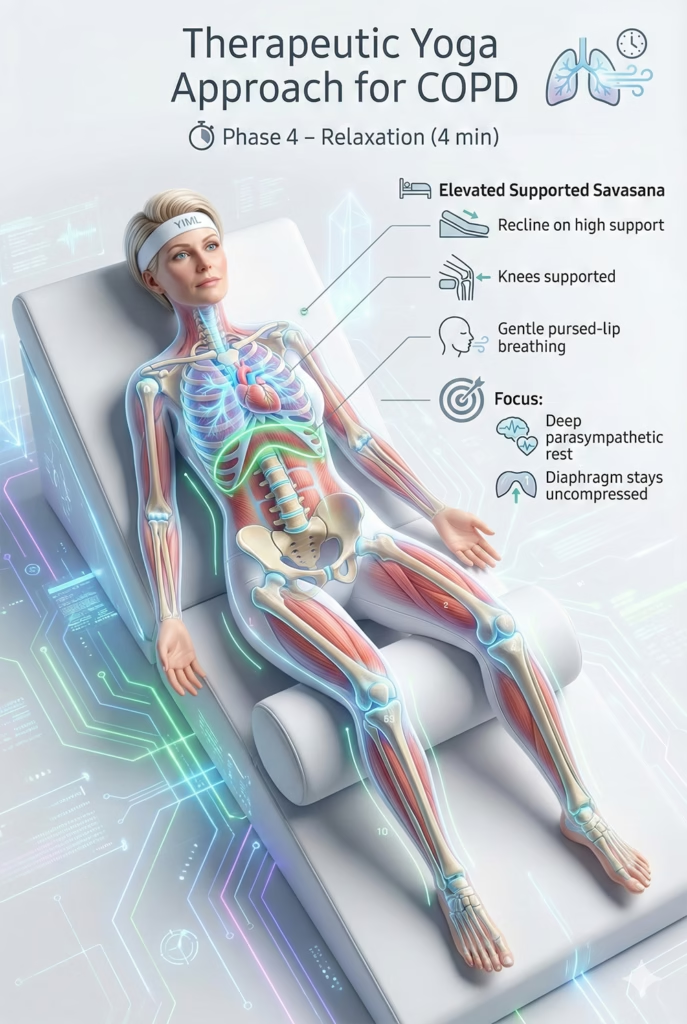
Phase 4: Total Systemic Relaxation (4 Minutes)
7. Elevated Supported Savasana
- Technique: Never lie flat. Sit on the floor/bed and lean back against a highly slanted stack of bolsters/pillows. Place a rolled blanket under the knees. Rest completely, maintaining gentle pursed-lip breathing.
- Goal: Induces profound parasympathetic rest while utilizing gravity to keep the diaphragm uncompressed.
Lifestyle & Ayurvedic Protocols for COPD
Daily Micro-Habits for Respiratory Hygiene The goal is to minimize mucus production (Kapha), reduce bronchial spasms (Vata), and optimize the mechanical environment for the lungs.
1. Daily Rhythm (Dinacharya)
- Sleep Posture: Always sleep with the head and shoulders elevated (using a wedge pillow or adjustable bed). Gravity assists diaphragmatic descent and prevents mucus pooling, reducing nocturnal dyspnea. Because nocturnal dyspnea frequently disrupts sleep architecture, emerging clinical evidence suggests that yoga-based interventions may help restore sleep quality and alleviate insomnia symptoms.
- The Gentle Rise: Do not jump out of bed. Sit up slowly. Perform 5-10 cycles of Pursed-Lip Breathing to clear the night’s trapped air before standing. Gentle chest percussion can aid expectoration.
- Targeted Abhyanga (Warm Oil Massage): Massage the chest, upper back, and neck with warm sesame oil infused with eucalyptus. The heat and oil pacify Vata spasms and relax hypertonic accessory muscles.
2. Energy Conservation (Pacing)
- Pacing is your most vital survival skill. Break tasks into smaller parts. Always exhale (via pursed lips) during the exertion phase of any movement (e.g., exhaling while standing up).
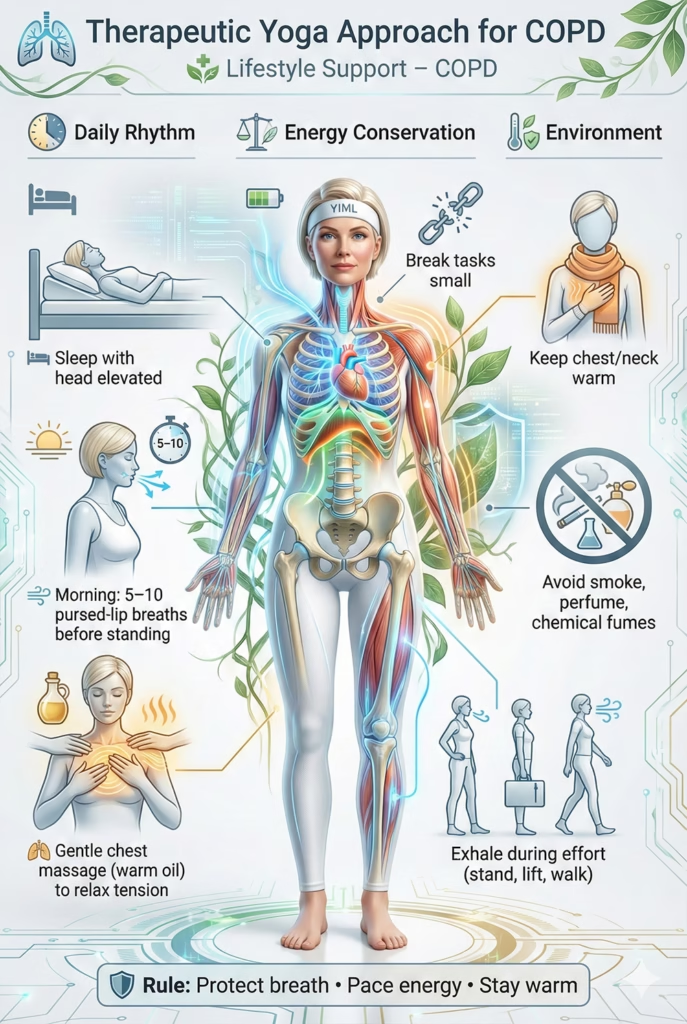
3. Environmental Precautions
- Stay Warm: Cold air is a potent trigger for severe bronchospasm (aggravating Vata and Kapha). Keep the neck and chest strictly protected in cold or air-conditioned environments.
- Avoid Irritants: Absolutely avoid smoke, strong perfumes, and chemical cleaners.
Ayurvedic Dietary Guidelines for COPD
COPD involves high Kapha (mucus/obstruction) and high Vata (dryness/spasm/tissue destruction). The diet must pacify Vata (warm, moist) while actively reducing Kapha (light, easy to digest) and strengthening Agni (digestive fire) to burn away Ama (mucus).
The Golden Rules
- Warm, Cooked, Light: Warmth soothes Vata spasms and melts Kapha mucus. Light, digestible foods prevent overloading Agni.
- Strictly Avoid Dairy & Sugar: These are the most potent Kapha-increasing foods and will rapidly increase thick mucus production.
Flavor Profiles (Rasa)
- Favor: Pungent (mildly spicy like ginger, black pepper—acts as an expectorant and warms the lungs), Bitter (leafy greens—dries up mucus), and Astringent (legumes).
- Avoid: Sweet (sugar, dairy, heavy fruits), Sour (fermented foods), and excessively Salty foods (causes fluid retention which strains the heart/lungs).
Healing Beverages
- Sip warm water constantly to keep mucus thin and easy to expectorate.
- Tulsi (Holy Basil) or Ginger Tea: Excellent Ayurvedic bronchodilators and expectorants.
Part V: Conclusion
Therapeutic Yoga offers a safe, scientifically validated, and highly comprehensive adjunctive approach to managing COPD. It shifts the paradigm from merely surviving breathless episodes to actively rehabilitating the mechanics of respiration.
By addressing the root mechanical failures—retraining the diaphragm, utilizing Pursed-Lip Breathing to stent airways and clear trapped air, and mobilizing a rigid ribcage—Yoga reduces the metabolic work of breathing. Simultaneously, through deep relaxation and mindfulness, it severs the neurological link between dyspnea and panic.
This journey requires immense patience, radical self-compassion, and strict adherence to your dyspnea threshold. Yoga does not cure the irreversible lung damage of COPD; rather, it empowers you to maximize the function of your remaining healthy tissue, reclaim control over your breath, and restore your quality of life.
Medical Disclaimer
IMPORTANT: The content provided in this article is for informational and educational purposes only. It is NOT intended to substitute for professional medical advice, diagnosis, or treatment.
- Always consult your pulmonologist or a qualified respiratory therapist regarding your COPD management.
- Never disregard professional medical advice or delay seeking it based on information read in this guide.
- Absolutely DO NOT alter or discontinue your prescribed inhalers, oxygen therapy, or oral medications without direct medical supervision.
References
Medical & Scientific Sources
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. (https://goldcopd.org/)
- American Lung Association. COPD. (https://www.lung.org/lung-health-diseases/lung-disease-lookup/copd)
- Holland, A. E., et al. (2012). Yoga for chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews.
- PubMed Central (National Library of Medicine). (https://www.ncbi.nlm.nih.gov/pmc/)
Yoga Therapy Sources
- McCall, T. (2007). Yoga as Medicine: The Yogic Prescription for Health and Healing. Bantam Dell.
- Saraswati, S. S. (2008). Asana Pranayama Mudra Bandha. Bihar School of Yoga.



