Part 1. Introduction
Chronic back pain is often cited as the “silent epidemic” of the 21st century. However, masked behind this generic term lies a spectrum of mechanical and physiological etiologies, each demanding a specialized treatment approach. One of the most specific and prevalent diagnoses is Lumbar Intervertebral Disc Prolapse (LIVDP), also known as Lumbar Disc Herniation (LDH). This condition occurs when the intervertebral discs—the spine’s “shock absorbers”—are damaged or degenerate, causing the nucleus pulposus to bulge or herniate, thereby directly compressing the spinal nerve roots.
The consequence is rarely just localized “mechanical” pain. Instead, it manifests as radicular pain with distinct characteristics: burning, electric-shock sensations, numbness, or paresthesia radiating along the nerve path into the buttocks and legs (commonly referred to as sciatica).
Treating LIVDP presents a significant challenge. Standard protocols typically commence with conservative measures: rest, pharmacotherapy (analgesics, anti-inflammatories, muscle relaxants), and physical therapy. When these fail, invasive interventions like epidural steroid injections or surgery may be considered. However, limitations abound: long-term medication use carries side effects, and invasive procedures bear inherent risks without guaranteed success. This creates an urgent need for non-invasive, safe, cost-effective, and efficacious treatments that empower patients to actively participate in their recovery.
Yoga, a holistic mind-body practice, has emerged as a promising solution. Theoretically, Yoga’s potential to address LIVDP is substantial. Yet, to transition this method from “alternative care” into the arsenal of Evidence-Based Medicine, a systematic synthesis and evaluation of existing research is required. This is the mission undertaken by this systematic review.
Research Overview
- English Title: The Impact of Yoga Therapy on Lumbar Intervertebral Disc Prolapse: A Systematic Review.
- Authors: Singh, AK et al.
- Year of Publication: 2024.
- DOI: 10.4103/ym.ym_26_24
Rationale for Selection
This review holds distinct value as it moves beyond “non-specific back pain” to focus on a specific structural diagnosis: LIVDP/LDH. This narrows the scope, providing highly applicable insights for a targeted patient group. Furthermore, as a Systematic Review, it adheres to PRISMA guidelines, ensuring transparency and comprehensiveness. By synthesizing data from various study types, it offers a panoramic view of current knowledge on this critical topic.
Part 2. Objectives and Hypothesis
Primary Objectives
The main goal of this systematic review is to evaluate and synthesize existing evidence regarding the efficacy of Yoga therapy on clinical outcomes in patients diagnosed with LIVDP/LDH. Specific objectives include:
- Synthesizing Study Types: Categorizing conducted research (RCTs, Case Studies, Quasi-experimental) and their characteristics.
- Evaluating Impact: Assessing Yoga’s effect on key patient and clinician outcomes, including disability levels, pain intensity, nerve conduction, and structural changes.
- Concluding & Directing: Determining Yoga’s position as a treatment option and identifying knowledge gaps to guide future research.

Scientific Hypothesis
Rather than testing a formal hypothesis, this review poses a research question: “Based on published literature, is Yoga therapy an effective and safe intervention for patients with lumbar disc herniation?” Implicitly, the review operates on the premise that evidence synthesis will reveal a positive trend supporting Yoga’s role.
Part 3. Methodology
Study Design
This is a Systematic Review following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines—an internationally recognized 27-item checklist ensuring the search, screening, extraction, and synthesis processes are transparent, systematic, and reproducible.
Subjects and Selection Criteria
- Data Sources: A comprehensive search was conducted across major medical databases (PubMed/Medline, Cochrane Library, Science Direct) and Google Scholar, covering the period from 2007 to 2024.
- Inclusion Criteria: Notably, the review adopted broad inclusion criteria:
- Randomized Controlled Trials (RCTs): The gold standard.
- Case Studies: Reports on individual or isolated cases.
- Quasi-experimental Studies: Intervention studies without randomization.
- Note: Including lower-level evidence allows for a broader scope but introduces limitations discussed later.
- Population: After screening, 10 articles met the criteria, encompassing a total of 546 patients.
Yoga Intervention
- Characteristics: The Yoga programs varied significantly across the 10 studies:
- Duration: Ranged from 3 weeks to 4 months.
- Frequency: Averaged ~2 sessions per week.
- Content: Typically Yoga Therapy, focusing on safe asanas, breathing techniques (Pranayama), and relaxation.
Clinical Measures (Key Outcomes)
The authors identified primary outcomes of interest, including:
- Disability Scores: e.g., Oswestry Disability Index (ODI).
- Pain Intensity: e.g., Visual Analog Scale (VAS).
- Nerve Conduction: Electrophysiological metrics to assess affected nerve root function.
- Structural Changes: Observable changes via imaging (MRI).

Part 4. Results
This systematic review synthesized findings from 10 studies, delivering a generally positive conclusion. As a narrative synthesis (not a meta-analysis), results are presented as trends rather than pooled statistical figures.
Key Findings Summary
1. Pain Intensity and Disability
This domain presents the most consistent evidence. Across the 10 analyzed studies (mean sample size 54.6; range 1–150), most research—from RCTs to case reports—recorded:
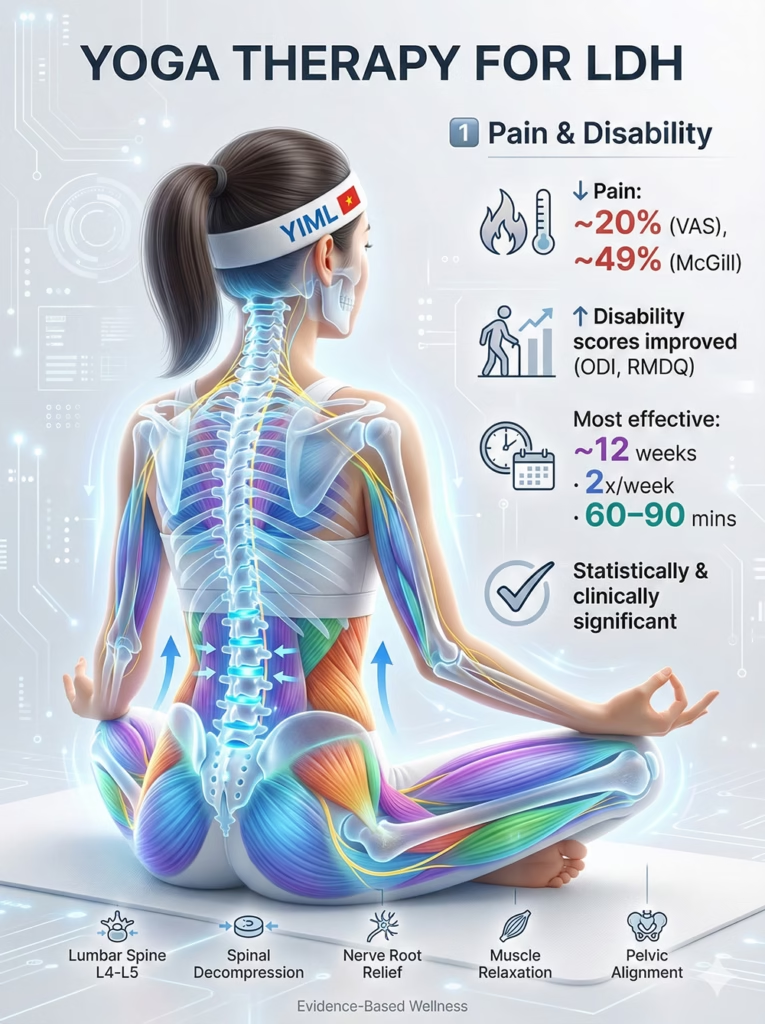
- Pain Reduction: ~20% decrease on the VAS scale.
- McGill Pain Questionnaire: ~49% reduction in scores.
- Significant Improvement in:
- Oswestry Disability Index (ODI).
- Roland–Morris Disability Questionnaire (RMDQ).
- Note: Reductions in pain and disability were statistically and clinically significant, particularly in programs lasting ~12 weeks (2 sessions/week, 60–90 mins/session).
2. Nerve Conduction and Structural Changes
Evidence for objective markers is scarcer but present:
- EMG: One case study showed improved nerve conduction after 21 days of residential yoga.
- MRI: A case-control study indicated lower disc degeneration in long-term yoga practitioners compared to non-practitioners.
- Flexibility: Increases in spinal Range of Motion (ROM).

3. Inflammatory Markers
Some studies noted positive shifts in biomarkers:
- Increase: β-endorphins (natural pain relief).
- Decrease: IL-6 and TNF-α (pro-inflammatory cytokines).
Statistical vs. Clinical Significance
- Statistical Significance: The general trend across 10 studies shows a positive, statistically significant correlation between Yoga practice and symptom remission.
- Clinical Significance: The overall conclusion positions Yoga Therapy as an effective, cost-efficient, and preventive strategy.
- Efficacy: Delivers on the two most critical treatment goals: pain reduction and functional improvement.
- Affordability: Compared to medical interventions, Yoga is cost-effective, especially in group settings.
- Prevention: By strengthening the core, improving posture, and enhancing somatic awareness, Yoga not only treats current pain but may prevent future recurrence.

Part 5. Discussion
The synthesized results paint a consistent and promising picture: Yoga therapy is an effective intervention for LIVDP. This discussion explores the multidimensional mechanisms through which Yoga “heals” LIVDP, validating the Biopsychosocial Model of chronic pain.
Mechanism 1: Biomechanical (The “Support Structure”)
- Core Strength & Spinal Stabilization: This is the foundational mechanism. Weakness in core muscles (transversus abdominis, deep back muscles, pelvic floor, diaphragm) is a primary driver of lumbar instability. Yoga therapy activates these muscles, creating a “natural corset” that stabilizes the lumbar spine, reduces micro-movements, and redistributes load, directly alleviating mechanical pressure on damaged discs.
- Decompression: Gentle axial extension postures in Yoga create minute spaces between vertebrae. While temporary, regular practice can reduce continuous compression on affected nerve roots.
- Flexibility & Muscle Balance: Radicular pain often triggers reflex spasms in surrounding muscles (hamstrings, hip flexors). Yoga provides controlled stretching to release these spasms, restoring postural balance.

Mechanism 2: Neurophysiological (“Rewriting” Pain Signals)
- Reducing Central Sensitization: In chronic pain, the central nervous system turns up the “volume” on pain signals. Yoga’s breathing (Pranayama) and relaxation techniques down-regulate the Sympathetic Nervous System and activate the Parasympathetic system. This deep relaxation helps “reset” the nervous system, reducing central sensitization.
- Cognitive Reframing: Through mindfulness, Yoga alters the patient’s relationship with pain. Observing pain as a sensation rather than a threat breaks the anxiety-pain cycle, significantly reducing the “suffering” component of pain.
While strong evidence already supports Yoga for non-specific chronic low back pain (Cochrane Review), emerging data suggest that carefully structured Yoga therapy may also benefit patients with lumbar disc herniation.
Limitations of the Evidence
While positive, the interpretation requires caution due to methodological limitations:
- Mixed Study Types: Combining RCTs (strong evidence) with case studies (weak evidence) risks overestimating efficacy.
- Sample Size: Small average sample sizes (~54) increase uncertainty and susceptibility to bias.
- Heterogeneity: The vast differences in Yoga protocols (duration, frequency, content) make it difficult to define a standard “dosage.”
- Lack of Objective Data: Benefits are primarily subjective (pain/function), with limited MRI or electrophysiological validation.
Implications for Practice
For physicians
Current evidence supports Yoga therapy as a structured, non-invasive adjunct within conservative management strategies for lumbar disc herniation.
Yoga should not be positioned as a replacement for medical care, but rather as:
- A symptom-modulating intervention (pain and disability reduction)
- A graded movement framework that supports functional restoration
- A patient-empowering self-management strategy

Referral considerations:
- Differentiate clearly between condition-specific therapeutic Yoga and general group-based fitness Yoga.
- Ensure instructors understand lumbar load management, radicular symptom monitoring, and progression principles.
- Encourage interdisciplinary collaboration where possible (physician–PT–Yoga therapist).
In this context, Yoga may enhance adherence to movement-based rehabilitation while minimizing long-term pharmacologic reliance.
Yoga Practice Application (Instructor’s Perspective)
This review offers supportive — though heterogeneous — evidence that Yoga can improve pain and function in individuals with LIVDP. However, therapeutic application demands specialization.
Working safely with this population requires:
- Functional understanding of lumbar biomechanics and disc pathology
- Ability to distinguish radicular pain from muscular stretch discomfort
- Clear awareness of contraindications (e.g., loaded deep lumbar flexion during acute symptomatic phases)
- Emphasis on spinal stability, motor control, and nervous system regulation before aggressive mobility work
Therapeutic priorities should include:
- Core stabilization and load distribution
- Symptom-guided progression
- Autonomic down-regulation to reduce pain amplification
The objective is not structural “disc correction,” but improved functional capacity, reduced pain perception, and enhanced long-term spinal resilience.
While systematic reviews clarify the efficacy profile of yoga for lumbar disc herniation, they do not provide granular implementation strategies. Clinicians and practitioners still require structured sequencing, load management principles, and safety-specific modifications to translate evidence into safe rehabilitation.
For a comprehensive therapeutic framework integrating biomechanical stabilization, neuromuscular re-education, breath regulation, and daily spinal hygiene protocols, refer to our structured clinical roadmap for lumbar disc herniation management.
Part 6. Conclusion
This systematic review synthesized evidence from 10 studies to conclude that Yoga therapy is an effective, cost-effective, and preventive treatment for patients with Lumbar Intervertebral Disc Prolapse (LIVDP) and general back pain. While the evidence quality is heterogeneous, there is a consistent trend of significant improvement in the most critical patient outcomes: pain intensity and disability levels.
However, this conclusion warrants cautious interpretation. Due to the mix of study designs and small sample sizes, larger-scale, high-quality Randomized Controlled Trials (RCTs) are needed to establish definitive clinical significance and standardize therapeutic protocols. Nevertheless, based on current evidence, Yoga has solidified its position as a valuable, promising non-invasive option in the comprehensive management of complex spinal conditions.
This article is part of our Research Decoded series within the Evidence-Informed Yoga Research Library.
References
- Singh, A. K., Singh, O. P., & N. K., S. (2024). The Impact of Yoga Therapy on Lumbar Intervertebral Disc Prolapse: A Systematic Review. Yoga Mimamsa, 56(2), 70.
- Gatchel, R. J., et al. (2007). The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychological Bulletin, 133(4), 581.
- Tekur, P., et al. (2022). A stretch and strength-based yoga exercise program for patients with neuropathic pain due to lumbar disc herniation: a randomized controlled trial. Spine, 47(1), 1-9.
![The Biomechanical Demands of Standing Yoga Poses in Seniors [RESEARCH DECODED]](https://yogaismylife.vn/en/wp-content/uploads/2026/02/tu-the-chien-binh-cho-nguoi-cao-tuoi.webp)
![The Impact of Yoga on Pediatric Obesity [RESEARCH DECODED]](https://yogaismylife.vn/en/wp-content/uploads/2026/02/The-Impact-of-Yoga-on-Pediatric-Obesity.avif)

